S-ar putea să vă placă și
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Cos Son 2015Document9 paginiCos Son 2015cintyaÎncă nu există evaluări
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Diabetes Metab RsumenesDocument6 paginiDiabetes Metab RsumenescintyaÎncă nu există evaluări
- Diabetes MetabDocument3 paginiDiabetes MetabcintyaÎncă nu există evaluări
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Cos Son 2015Document13 paginiCos Son 2015cintyaÎncă nu există evaluări
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Respiratory System - AnatomyDocument28 paginiRespiratory System - AnatomyDinesh KumarÎncă nu există evaluări
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Health Care in Global 2018 PDFDocument36 paginiHealth Care in Global 2018 PDFTony Miguel Saba SabaÎncă nu există evaluări
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- Necrosis and Types of NecrosisDocument2 paginiNecrosis and Types of NecrosisHisham NesemÎncă nu există evaluări
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Human Malformations - 07 - SkullDocument46 paginiHuman Malformations - 07 - SkullAhmed H. Ali ElbestaweyÎncă nu există evaluări
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
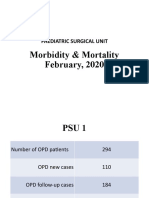
- Morbidity & Mortality (February, 2020)Document14 paginiMorbidity & Mortality (February, 2020)Wai GyiÎncă nu există evaluări
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- ABCDE Approach To The Critically Ill Patient - Nick SmithDocument40 paginiABCDE Approach To The Critically Ill Patient - Nick SmithBadrul Hisyam Alias100% (1)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Seminar On Fluid-and-Electrolyte-ImbalanceDocument35 paginiSeminar On Fluid-and-Electrolyte-Imbalancemohamad dildarÎncă nu există evaluări
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Maye Bato 47 Yo, F: Surgery Module 5 Facilitator: Dr. Jerry Alinsug Group 7Document1 paginăMaye Bato 47 Yo, F: Surgery Module 5 Facilitator: Dr. Jerry Alinsug Group 7Luke Matthew MondaresÎncă nu există evaluări
- Key Answers On The ExamDocument81 paginiKey Answers On The ExamKarl Kiw-isÎncă nu există evaluări
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- Review Notes For Diabetes MellitusDocument8 paginiReview Notes For Diabetes MellitusEditha LucasÎncă nu există evaluări
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Oxford Handbook of Clinical Pathology PDFDocument7 paginiOxford Handbook of Clinical Pathology PDFppgpcsÎncă nu există evaluări
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- RN MedSurgDocument685 paginiRN MedSurgArgyll Baye Ansuas100% (4)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- Organ Systems Practice TestDocument8 paginiOrgan Systems Practice TestChristine RomanillosÎncă nu există evaluări
- Krok 2 Medicine (EN) Attempt Review 1Document52 paginiKrok 2 Medicine (EN) Attempt Review 1IS ZDÎncă nu există evaluări
- Cardiac Pacemaker: BY E.DeepikaDocument17 paginiCardiac Pacemaker: BY E.Deepikadeepika_164Încă nu există evaluări
- Rate P Wave QRS Comple X PR Interval: ST RDDocument2 paginiRate P Wave QRS Comple X PR Interval: ST RDPat G.Încă nu există evaluări
- Eval Microcir Curr - Op.cc 23Document8 paginiEval Microcir Curr - Op.cc 23Julian SanchezÎncă nu există evaluări
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Emergency Management of Cardiac Chest Pain: A ReviewDocument5 paginiEmergency Management of Cardiac Chest Pain: A Reviewahmad habibÎncă nu există evaluări
- Project #7 - HypertensionDocument2 paginiProject #7 - HypertensionKPÎncă nu există evaluări
- Predicting Heart Disease at Early Stages Using Machine Learning: A SurveyDocument4 paginiPredicting Heart Disease at Early Stages Using Machine Learning: A SurveyLucas FiordelisiÎncă nu există evaluări
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Chronic Kidney Disease in Adults - Assessment and ManagementDocument5 paginiChronic Kidney Disease in Adults - Assessment and ManagementAnahí Cortés HerreraÎncă nu există evaluări
- PHC Answers Class 38Document36 paginiPHC Answers Class 38لآلئ القرآنÎncă nu există evaluări
- Aew 214Document11 paginiAew 214Heather PorterÎncă nu există evaluări
- Dipiro DislipidemiaDocument49 paginiDipiro DislipidemiaMila ErnilaÎncă nu există evaluări
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (120)
- Cardiologia Croatica 2021 16 - 1-2 - 83Document1 paginăCardiologia Croatica 2021 16 - 1-2 - 83daia4322746Încă nu există evaluări
- DefinitionDocument9 paginiDefinitionKhondokar ArafatÎncă nu există evaluări
- PDA Case StudyDocument5 paginiPDA Case StudyDiana Andrea AyongaoÎncă nu există evaluări
- YR 4 Lecture Urogenital ImagingDocument59 paginiYR 4 Lecture Urogenital ImagingMUBIRU SAMUEL EDWARDÎncă nu există evaluări
- Introduction To Global Health 2nd Edition Jacobsen Test BankDocument5 paginiIntroduction To Global Health 2nd Edition Jacobsen Test Banksinhhanhi7rp100% (28)
- Tracheobronchial Tree and Bronchopulmonary SegmentsDocument60 paginiTracheobronchial Tree and Bronchopulmonary SegmentsSathya RajaÎncă nu există evaluări
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)