S-ar putea să vă placă și
- Resolving Attachment Injuries in Couples Using Emotionally Focused Therapy: A Three-Year Follow-UpDocument18 paginiResolving Attachment Injuries in Couples Using Emotionally Focused Therapy: A Three-Year Follow-UpEFTcouplesÎncă nu există evaluări
- Emotionally Focused Family Therapy: Developing The ModelDocument9 paginiEmotionally Focused Family Therapy: Developing The ModelEFTcouplesÎncă nu există evaluări
- Emotionally Focused Therapy (Eft) and Emotionally Focused Family Therapy (Efft) : A Challenge/opportunity For Systemic and Post-Systemic TherapistsDocument5 paginiEmotionally Focused Therapy (Eft) and Emotionally Focused Family Therapy (Efft) : A Challenge/opportunity For Systemic and Post-Systemic TherapistsEFTcouplesÎncă nu există evaluări
- EFT ResearchDocument5 paginiEFT ResearchEFTcouplesÎncă nu există evaluări
- A Socio-Emotional Approach To Couple Therapy: Linking Social Context and Couple InteractionDocument17 paginiA Socio-Emotional Approach To Couple Therapy: Linking Social Context and Couple InteractionEFTcouplesÎncă nu există evaluări
- Critical Incidents That Help and Hinder Learning Emotionally Focused Therapy For CouplesDocument19 paginiCritical Incidents That Help and Hinder Learning Emotionally Focused Therapy For CouplesEFTcouplesÎncă nu există evaluări
- Narrative Change in Emotion-Focused Therapy: How Is Change Constructed Through The Lens of The Innovative Moments Coding System?Document11 paginiNarrative Change in Emotion-Focused Therapy: How Is Change Constructed Through The Lens of The Innovative Moments Coding System?EFTcouplesÎncă nu există evaluări
- Treating Attachment Injured Couples With Emotionally Focused Therapy - A Case Study ApproachDocument24 paginiTreating Attachment Injured Couples With Emotionally Focused Therapy - A Case Study ApproachEFTcouplesÎncă nu există evaluări
- The Construction of A Model of The Process of Couples' Forgiveness in Emotion-Focused Therapy For CouplesDocument13 paginiThe Construction of A Model of The Process of Couples' Forgiveness in Emotion-Focused Therapy For CouplesEFTcouplesÎncă nu există evaluări
- The Experience of Learning Emotionally Focused Couples TherapyDocument19 paginiThe Experience of Learning Emotionally Focused Couples TherapyEFTcouplesÎncă nu există evaluări
- What Works For Whom - A Meta-Analytic Review of Marital and Couples Therapy in Reference To Marital DistressDocument16 paginiWhat Works For Whom - A Meta-Analytic Review of Marital and Couples Therapy in Reference To Marital DistressEFTcouplesÎncă nu există evaluări
- Supervising Emotionally Focused Therapists - A Systematic Research-Based ModelDocument17 paginiSupervising Emotionally Focused Therapists - A Systematic Research-Based ModelEFTcouplesÎncă nu există evaluări
- The Efficacy of Emotionally Focused Couple Therapy (EFT-C) Training With Regard To Reducing Sexual Dissatisfaction Among CouplesDocument9 paginiThe Efficacy of Emotionally Focused Couple Therapy (EFT-C) Training With Regard To Reducing Sexual Dissatisfaction Among CouplesEFTcouplesÎncă nu există evaluări
- The Path To A Secure Bond - Emotionally Focused Couple TherapyDocument14 paginiThe Path To A Secure Bond - Emotionally Focused Couple TherapyEFTcouples100% (1)
- The Efficacy of Behavioral Couples Therapy and Emotionally Focused Therapy For Couple DistressDocument28 paginiThe Efficacy of Behavioral Couples Therapy and Emotionally Focused Therapy For Couple DistressEFTcouplesÎncă nu există evaluări
- Forgiveness and The Appraisal-Coping Process in Response To Relationship Conflicts - Implications For Depressive SymptomsDocument16 paginiForgiveness and The Appraisal-Coping Process in Response To Relationship Conflicts - Implications For Depressive SymptomsEFTcouplesÎncă nu există evaluări
- The Dynamics of Emotion, Love and Power in An Emotion-Focused Approach To Couple TherapyDocument16 paginiThe Dynamics of Emotion, Love and Power in An Emotion-Focused Approach To Couple TherapyEFTcouplesÎncă nu există evaluări
- Short-Term and Long-Term Effects of Training in Emotionally Focused Couple Therapy - Professional and Personal AspectsDocument14 paginiShort-Term and Long-Term Effects of Training in Emotionally Focused Couple Therapy - Professional and Personal AspectsEFTcouplesÎncă nu există evaluări
- Depression TherapyDocument34 paginiDepression Therapysymval100% (1)
- Perceptions of Attachment Style and Marital Quality in Midlife MarriageDocument13 paginiPerceptions of Attachment Style and Marital Quality in Midlife MarriageEFTcouplesÎncă nu există evaluări
- Integration of A Cultural Lens With Emotionally Focused TherapyDocument13 paginiIntegration of A Cultural Lens With Emotionally Focused TherapyEFTcouplesÎncă nu există evaluări
- Contrasting Two Clients in Emotion-Focused Therapy For Depression - The Case of "Tom," "Trapped in The Tunnel"Document38 paginiContrasting Two Clients in Emotion-Focused Therapy For Depression - The Case of "Tom," "Trapped in The Tunnel"EFTcouplesÎncă nu există evaluări
- Emotion-Focused Couples Therapy and The Facilitation of ForgivenessDocument16 paginiEmotion-Focused Couples Therapy and The Facilitation of ForgivenessEFTcouplesÎncă nu există evaluări
- Emotionally Focused Therapy For Couples and Childhood Sexual Abuse SurvivorsDocument19 paginiEmotionally Focused Therapy For Couples and Childhood Sexual Abuse SurvivorsEFTcouplesÎncă nu există evaluări
- Emotionally Focused Couples Therapy - Status and ChallengesDocument13 paginiEmotionally Focused Couples Therapy - Status and ChallengesEFTcouplesÎncă nu există evaluări
- Emotion-Focused Therapy For Couples in The Treatment of Depression - A Pilot StudyDocument11 paginiEmotion-Focused Therapy For Couples in The Treatment of Depression - A Pilot StudyEFTcouples100% (1)
- Couples and Chronic Illness: An Attachment Perspective and Emotionally Focused Therapy InterventionsDocument17 paginiCouples and Chronic Illness: An Attachment Perspective and Emotionally Focused Therapy InterventionsEFTcouplesÎncă nu există evaluări
- A Socio-Emotional Approach To Couple Therapy: Linking Social Context and Couple InteractionDocument17 paginiA Socio-Emotional Approach To Couple Therapy: Linking Social Context and Couple InteractionEFTcouplesÎncă nu există evaluări
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (587)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (265)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (119)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Specialized Connective TissueDocument15 paginiSpecialized Connective TissueSebÎncă nu există evaluări
- Power Systems-III Ditital NotesDocument102 paginiPower Systems-III Ditital NotesSimranÎncă nu există evaluări
- Cswip Visual Welding Inspector 3.0 BrochureDocument1 paginăCswip Visual Welding Inspector 3.0 BrochureNasfauzan100% (2)
- DSUSJRC01161350 Corail ST-Total Hip SystemDocument20 paginiDSUSJRC01161350 Corail ST-Total Hip SystemXeniaÎncă nu există evaluări
- 21 - Effective Pages: Beechcraft CorporationDocument166 pagini21 - Effective Pages: Beechcraft CorporationCristian PugaÎncă nu există evaluări
- Yanagiba Sharpening: Everything You Need To KnowDocument16 paginiYanagiba Sharpening: Everything You Need To KnowT ChenÎncă nu există evaluări
- BOD FormatDocument4 paginiBOD FormatSkill IndiaÎncă nu există evaluări
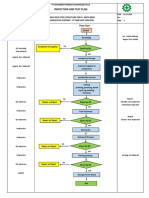
- Inspection and Test Plan: Flow Chart Start IncomingDocument1 paginăInspection and Test Plan: Flow Chart Start IncomingSinden AyuÎncă nu există evaluări
- 0001 CatDocument108 pagini0001 CatJorge CabreraÎncă nu există evaluări
- Ficha Tecnica StyrofoamDocument2 paginiFicha Tecnica StyrofoamAceroMart - Tu Mejor Opcion en AceroÎncă nu există evaluări
- Radioimmunoassay MarketDocument5 paginiRadioimmunoassay MarketRajni GuptaÎncă nu există evaluări
- Seguridad Boltec Cable PDFDocument36 paginiSeguridad Boltec Cable PDFCesar QuintanillaÎncă nu există evaluări
- Lesson 5 - The Problem of EvilDocument10 paginiLesson 5 - The Problem of Evilsemmerson4896Încă nu există evaluări
- Eltra Cs 530Document122 paginiEltra Cs 530ahalonsoÎncă nu există evaluări
- Project Report On Air FilterDocument5 paginiProject Report On Air FilterEIRI Board of Consultants and PublishersÎncă nu există evaluări
- Bespoke Fabrication Systems for Unique Site SolutionsDocument13 paginiBespoke Fabrication Systems for Unique Site Solutionswish uÎncă nu există evaluări
- Asme NM.2-2018Document126 paginiAsme NM.2-2018aneeshjokay75% (4)
- Evolution Chart 3Document1 paginăEvolution Chart 3sasupraÎncă nu există evaluări
- Keys To Biblical CounselingDocument7 paginiKeys To Biblical CounselingDavid Salazar100% (6)
- Baileys in 2009: Case Study Reference No 509-050-1Document17 paginiBaileys in 2009: Case Study Reference No 509-050-1Ernesto KulasinÎncă nu există evaluări
- AnxietyDocument5 paginiAnxietydrmadankumarbnysÎncă nu există evaluări
- 6V Plush Ride-On: Owner'S ManualDocument26 pagini6V Plush Ride-On: Owner'S ManualVisas LaredoÎncă nu există evaluări
- Stepan Formulation 943Document2 paginiStepan Formulation 943Mohamed AdelÎncă nu există evaluări
- Performance and Mechanical Running Tests of Centrifugal CompressorsDocument5 paginiPerformance and Mechanical Running Tests of Centrifugal CompressorsVicky KumarÎncă nu există evaluări
- Cement Evaluation CAST-CBL HalliburtonDocument36 paginiCement Evaluation CAST-CBL HalliburtonrezaÎncă nu există evaluări
- GDCR Final PDFDocument311 paginiGDCR Final PDFHrushikesh PatelÎncă nu există evaluări
- PE 560 Atomic Absorption Spectrophotometer ManualDocument176 paginiPE 560 Atomic Absorption Spectrophotometer ManualDavid Allan100% (1)
- CanteenDocument8 paginiCanteenmahesh4uÎncă nu există evaluări
- Sampling & Data AssayDocument22 paginiSampling & Data AssayFerdinand SiahaanÎncă nu există evaluări
- Fluvial Erosion Processes ExplainedDocument20 paginiFluvial Erosion Processes ExplainedPARAN, DIOSCURAÎncă nu există evaluări