S-ar putea să vă placă și
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Hahnemann S., Chronic DisDocument167 paginiHahnemann S., Chronic Dishompat100% (1)
- Responsive Document - CREW: FDA: Regarding Communications Between The FDA and Martin Shkreli: 11/30/2012 - 11005576 - Enc - EJLDocument12 paginiResponsive Document - CREW: FDA: Regarding Communications Between The FDA and Martin Shkreli: 11/30/2012 - 11005576 - Enc - EJLCREWÎncă nu există evaluări
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Psoriatic ArthritisDocument10 paginiPsoriatic ArthritisSaba AyurvedaÎncă nu există evaluări
- NCP: Chronic Obstructive Pulmonary Disease and AsthmaDocument15 paginiNCP: Chronic Obstructive Pulmonary Disease and AsthmaJavie100% (5)
- Prolonged PregnancyDocument40 paginiProlonged Pregnancyjan caraÎncă nu există evaluări
- NCP PretermDocument5 paginiNCP PretermJamine Joyce Ortega-AlvarezÎncă nu există evaluări
- Emergency Room PoliciesDocument3 paginiEmergency Room PoliciesEduardo Anerdez100% (6)
- Accessory TragusDocument3 paginiAccessory TragusDeba P SarmaÎncă nu există evaluări
- Acantholytic Dermatosis With DyskeratosisDocument11 paginiAcantholytic Dermatosis With DyskeratosisDeba P SarmaÎncă nu există evaluări
- Pilar Cyst With CrystalsDocument2 paginiPilar Cyst With CrystalsDeba P SarmaÎncă nu există evaluări
- Acantholytic Solar Keratosis, M 67, Forehead PDFDocument6 paginiAcantholytic Solar Keratosis, M 67, Forehead PDFDeba P SarmaÎncă nu există evaluări
- Acantholytic Bullous DiseaseDocument4 paginiAcantholytic Bullous DiseaseDeba P SarmaÎncă nu există evaluări
- Acantholytic Actinic KeratosisDocument4 paginiAcantholytic Actinic KeratosisDeba P SarmaÎncă nu există evaluări
- Acantholytic Bullous Disease (Darier's Disease, Keratosis Follicularis)Document3 paginiAcantholytic Bullous Disease (Darier's Disease, Keratosis Follicularis)Deba P SarmaÎncă nu există evaluări
- Xanthogranuloma PPT DSDocument9 paginiXanthogranuloma PPT DSDeba P SarmaÎncă nu există evaluări
- Acantholytic Acanthoma. M 60, ScrotumDocument8 paginiAcantholytic Acanthoma. M 60, ScrotumDeba P SarmaÎncă nu există evaluări
- Results of Search in Google Scholar On 'Deba P Sarma'Document28 paginiResults of Search in Google Scholar On 'Deba P Sarma'Deba P SarmaÎncă nu există evaluări
- Balanitis Circumscripta Plasmacellularis (Zoon's Balanitis, Plasma Cell Balanitis)Document6 paginiBalanitis Circumscripta Plasmacellularis (Zoon's Balanitis, Plasma Cell Balanitis)Deba P SarmaÎncă nu există evaluări
- Xanthomatous Synovial Cyst (Xanthomatous Ganglion Cyst), M 74, Left PalmDocument7 paginiXanthomatous Synovial Cyst (Xanthomatous Ganglion Cyst), M 74, Left PalmDeba P SarmaÎncă nu există evaluări
- Xanthogranuloma, M 30, Right ElbowDocument4 paginiXanthogranuloma, M 30, Right ElbowDeba P SarmaÎncă nu există evaluări
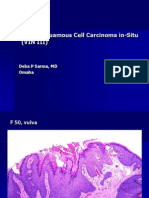
- Vulvar Squamous Cell Carcinoma In-Situ (VIN III), F 50, VulvaDocument6 paginiVulvar Squamous Cell Carcinoma In-Situ (VIN III), F 50, VulvaDeba P SarmaÎncă nu există evaluări
- Verrucous Epidermal Nevus. F 43, ScalpDocument4 paginiVerrucous Epidermal Nevus. F 43, ScalpDeba P SarmaÎncă nu există evaluări
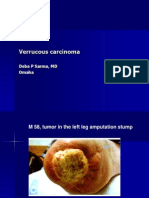
- Verrucous Carcinoma., M 58, Left Leg Amputation StumpDocument7 paginiVerrucous Carcinoma., M 58, Left Leg Amputation StumpDeba P SarmaÎncă nu există evaluări
- Verrucous Carcinoma of The Foot, M 63, Left FootDocument8 paginiVerrucous Carcinoma of The Foot, M 63, Left FootDeba P Sarma100% (1)
- Verruca Vulgaris., M 22.,PPTDocument2 paginiVerruca Vulgaris., M 22.,PPTDeba P SarmaÎncă nu există evaluări
- Marketing Pharmaceutical CareDocument12 paginiMarketing Pharmaceutical CareTri Hilma Pertiwi100% (1)
- 1-Evidence Based Midwifery Care PDFDocument11 pagini1-Evidence Based Midwifery Care PDFsinarÎncă nu există evaluări
- Medicine 2Document1 paginăMedicine 2aasi121Încă nu există evaluări
- Low Back Pain Among Medical StudentsDocument6 paginiLow Back Pain Among Medical StudentsMirza Kurnia AngelitaÎncă nu există evaluări
- Community Health Nursing BulletsDocument5 paginiCommunity Health Nursing BulletsDefensor Pison GringgoÎncă nu există evaluări
- Natural Remedies For Bacterial OvergrowthDocument15 paginiNatural Remedies For Bacterial OvergrowthRobit SiddikiÎncă nu există evaluări
- 37 - Hematuria & RCCDocument53 pagini37 - Hematuria & RCCRashed ShatnawiÎncă nu există evaluări
- Medical Fitness Certificate FORMATDocument2 paginiMedical Fitness Certificate FORMATpriyanshuÎncă nu există evaluări
- Aphthous Stomatitis - Background, Pathophysiology, EpidemiologyDocument8 paginiAphthous Stomatitis - Background, Pathophysiology, EpidemiologyRizalRyamizardÎncă nu există evaluări
- Letter and Nurse)Document2 paginiLetter and Nurse)ruggero07Încă nu există evaluări
- CPCR NewDocument30 paginiCPCR NewPhil PhilipsÎncă nu există evaluări
- Presentasi ScabiesDocument21 paginiPresentasi ScabiesMunawwar AwaÎncă nu există evaluări
- NCP Diabetes MellitusDocument2 paginiNCP Diabetes MellitusrhueneisenÎncă nu există evaluări
- Lusensi Periapikal Panoramik-BF-1 Juli 2020Document19 paginiLusensi Periapikal Panoramik-BF-1 Juli 2020Roberto HutapeaÎncă nu există evaluări
- History of Neurosurgery in IndonesiaDocument23 paginiHistory of Neurosurgery in IndonesiaPetra O.P. WahjoePramonoÎncă nu există evaluări
- PolDocument34 paginiPollouise VincoÎncă nu există evaluări
- Pressure Ulcer Prevention in Long Term CareDocument6 paginiPressure Ulcer Prevention in Long Term CareambariyantoÎncă nu există evaluări
- Ghayathi Hospital Applicant Online Interview 2016Document4 paginiGhayathi Hospital Applicant Online Interview 2016Kathleen ValinadoÎncă nu există evaluări
- Chapter 10: Elimination Test Bank: 1. A. B. C. D. Ans: ADocument6 paginiChapter 10: Elimination Test Bank: 1. A. B. C. D. Ans: AMary SingletonÎncă nu există evaluări
- Aggressive Adenomatoid Odontogenic Tumor of Maxilla Involving Impacted Third Molar - A Rare Case ReportDocument7 paginiAggressive Adenomatoid Odontogenic Tumor of Maxilla Involving Impacted Third Molar - A Rare Case ReportRisyaRahmadaniÎncă nu există evaluări
- Strategic Preparedness and Response PlanDocument28 paginiStrategic Preparedness and Response PlanPeter MeierÎncă nu există evaluări
- Rapid AbgDocument11 paginiRapid AbgDeoMikhailAngeloNuñezÎncă nu există evaluări
- NCD High-Risk Assessment (Community Case Finding Form) NCD High-Risk Assessment (Community Case Finding Form)Document1 paginăNCD High-Risk Assessment (Community Case Finding Form) NCD High-Risk Assessment (Community Case Finding Form)Gen GenÎncă nu există evaluări