S-ar putea să vă placă și
- Cross-Training: The Medical Assistant WorkbookDe la EverandCross-Training: The Medical Assistant WorkbookÎncă nu există evaluări
- Kochi Claim FormDocument4 paginiKochi Claim FormRadhika ShenoiÎncă nu există evaluări
- Mdindia Healthcare Services (Tpa) Pvt. LTD.: Claim FormDocument5 paginiMdindia Healthcare Services (Tpa) Pvt. LTD.: Claim FormrhvenkatÎncă nu există evaluări
- Documentation for Skilled Nursing & Long-Term Care: A Guide for Occupational TherapistsDe la EverandDocumentation for Skilled Nursing & Long-Term Care: A Guide for Occupational TherapistsÎncă nu există evaluări
- Claim FormDocument5 paginiClaim Formsoumyadeep19478425Încă nu există evaluări
- Mdindia Healthcare Services (Tpa) Pvt. LTD.: Claim FormDocument4 paginiMdindia Healthcare Services (Tpa) Pvt. LTD.: Claim FormShubakar ReddyÎncă nu există evaluări
- Others Claim FormDocument5 paginiOthers Claim FormArvind RayÎncă nu există evaluări
- Mdindia Healthcare Services (Tpa) Pvt. LTD.: Claim FormDocument4 paginiMdindia Healthcare Services (Tpa) Pvt. LTD.: Claim FormDeepakÎncă nu există evaluări
- Kolkata Claim Form - MD-IndiaDocument4 paginiKolkata Claim Form - MD-Indiadipankar0majumderÎncă nu există evaluări
- Adamjee Insurance Company Limited: Health Insurance - In-Patient Claim FormDocument2 paginiAdamjee Insurance Company Limited: Health Insurance - In-Patient Claim FormubaidÎncă nu există evaluări
- In-Patient Claim FormDocument2 paginiIn-Patient Claim Formfaisal_1241Încă nu există evaluări
- MediHub Request For Letter of Guarantee Form 2021 v2 2 1 - 1Document2 paginiMediHub Request For Letter of Guarantee Form 2021 v2 2 1 - 1Lhogeswaran RaviÎncă nu există evaluări
- National Inurance Company Limited - Claim FormDocument3 paginiNational Inurance Company Limited - Claim FormfuckyouprettyÎncă nu există evaluări
- Medical Attendant S/ Hospital Certificate: (Format AI - Death Claim)Document2 paginiMedical Attendant S/ Hospital Certificate: (Format AI - Death Claim)PiyushÎncă nu există evaluări
- Peace Corps Alcohol/Substance Abuse Current Evaluation Form PC-262-6 (Initial Approval 08/2012Document5 paginiPeace Corps Alcohol/Substance Abuse Current Evaluation Form PC-262-6 (Initial Approval 08/2012Accessible Journal Media: Peace Corps DocumentsÎncă nu există evaluări
- Mediclaim FormDocument1 paginăMediclaim Formpicrush2pmÎncă nu există evaluări
- New Patient Information-2021Document6 paginiNew Patient Information-2021Anime300Încă nu există evaluări
- Head Office: 87, M G Road, Fort, Mumbai-400001: I. II - CLAIM NO.Document5 paginiHead Office: 87, M G Road, Fort, Mumbai-400001: I. II - CLAIM NO.gaddipati_ramuÎncă nu există evaluări
- MD India Insurance Claim FormDocument5 paginiMD India Insurance Claim FormYogesh ParchaniÎncă nu există evaluări
- Medical Information FormDocument1 paginăMedical Information FormmpriceatccusaÎncă nu există evaluări
- NAIC Claim Form PDFDocument3 paginiNAIC Claim Form PDFMohit BaggaÎncă nu există evaluări
- GMC Claim Form How To File A ClaimDocument4 paginiGMC Claim Form How To File A ClaimtweetknotÎncă nu există evaluări
- 08 Claim FormDocument4 pagini08 Claim Formanurag1309Încă nu există evaluări
- General Consent For Treatment Form Oct 2016Document2 paginiGeneral Consent For Treatment Form Oct 2016Dewi Ratna SariÎncă nu există evaluări
- Group and Individual Medical Claims FormDocument3 paginiGroup and Individual Medical Claims FormSheikh Alif Amzar BuxÎncă nu există evaluări
- Claim Form-MD IndiaDocument5 paginiClaim Form-MD IndiaMusycal FynncÎncă nu există evaluări
- Patient Registration Form 13Document4 paginiPatient Registration Form 13windawaty humolaÎncă nu există evaluări
- DHS DHS: Dedicated Healthcare Services (India) Private LimitedDocument1 paginăDHS DHS: Dedicated Healthcare Services (India) Private Limiteddisk_la_poduÎncă nu există evaluări
- Toddler QuestionaireDocument3 paginiToddler Questionaireanarki85Încă nu există evaluări
- Health Insurance Claim FormDocument3 paginiHealth Insurance Claim FormdivechahimanshuÎncă nu există evaluări
- Form 070324Document2 paginiForm 070324Arid AgricultureÎncă nu există evaluări
- Claim Form IHealthcareDocument5 paginiClaim Form IHealthcarePradeep Kumar VupalaÎncă nu există evaluări
- Dental WaiverDocument1 paginăDental WaiverMary Grace LemonÎncă nu există evaluări
- UIICHdfc ClaimformDocument2 paginiUIICHdfc ClaimformdomyomglolÎncă nu există evaluări
- Memorial Hermann Discharge Papers - 3Document5 paginiMemorial Hermann Discharge Papers - 3Alaska JamesÎncă nu există evaluări
- Crewsure Claim Form (XLCatlin) 1.3Document2 paginiCrewsure Claim Form (XLCatlin) 1.3Andrei Belehuzi0% (1)
- National Insurance Company LimitedDocument4 paginiNational Insurance Company Limitedkaransandesara777Încă nu există evaluări
- CDC Data Collection Long FormDocument13 paginiCDC Data Collection Long FormBanzai Health Private LimitedÎncă nu există evaluări
- Claims Form For New India AssuranceDocument2 paginiClaims Form For New India AssuranceRafael BlackÎncă nu există evaluări
- Patient Information Sheet 091409Document2 paginiPatient Information Sheet 091409api-16816262Încă nu există evaluări
- Cooperative Health Management Federation: Enrollment Application Form (Eaf)Document2 paginiCooperative Health Management Federation: Enrollment Application Form (Eaf)Geraldine Daquipil TortalÎncă nu există evaluări
- ClaimDocument1 paginăClaimStephen JoyÎncă nu există evaluări
- Advocare Consent Disclosure Authorization PDFDocument2 paginiAdvocare Consent Disclosure Authorization PDFAsnaifa Bint MamintalÎncă nu există evaluări
- PT FormsDocument2 paginiPT Formsmerengue100Încă nu există evaluări
- New Patient RegistrationDocument2 paginiNew Patient Registrationnaveenmi2100% (1)
- Adult Intake-1Document13 paginiAdult Intake-1Kimberly StanfordÎncă nu există evaluări
- Authorization of Temporary Guardianship: The Parties To This Agreement AreDocument2 paginiAuthorization of Temporary Guardianship: The Parties To This Agreement ArefelixÎncă nu există evaluări
- Medical Claim Form (Reimbursement Only)Document2 paginiMedical Claim Form (Reimbursement Only)Muhammad Rizwan Tariq100% (1)
- Acupuncture Intake FormDocument2 paginiAcupuncture Intake FormMeraki MaryÎncă nu există evaluări
- Fixed Claim FormDocument2 paginiFixed Claim FormVikas GiriÎncă nu există evaluări
- (IL) FMLA Certification Form Employee Condition Beatriz RuizDocument5 pagini(IL) FMLA Certification Form Employee Condition Beatriz RuizBeatriz RuizÎncă nu există evaluări
- BSIB GHS Claim FormDocument3 paginiBSIB GHS Claim FormmuhsinmohammedÎncă nu există evaluări
- SBIL - Health QuestionnaireDocument2 paginiSBIL - Health QuestionnaireKrishna GBÎncă nu există evaluări
- Clinical Volunteer ApplicationDocument3 paginiClinical Volunteer ApplicationAnonymous tS0WWCCÎncă nu există evaluări
- Preauthorization Request Form - FinalDocument3 paginiPreauthorization Request Form - FinalRiya GhayelÎncă nu există evaluări
- Psychiatric Admission EvaluationDocument5 paginiPsychiatric Admission Evaluationfernlover3901Încă nu există evaluări
- Bajaj Allianz Cashless Request FormDocument3 paginiBajaj Allianz Cashless Request FormM/s MicrotechÎncă nu există evaluări
- Proposal Form Ashakiran PDFDocument6 paginiProposal Form Ashakiran PDFSreejith Rajendran PillaiÎncă nu există evaluări
- PATIENT INFORMATION - Please Fill Out CompletelyDocument5 paginiPATIENT INFORMATION - Please Fill Out CompletelynorniellarÎncă nu există evaluări
- Grades 7-9 Life Orientation CapsDocument27 paginiGrades 7-9 Life Orientation CapsngeleÎncă nu există evaluări
- Research Bio StratchDocument48 paginiResearch Bio StratchJanuar Dwi YudhistiraÎncă nu există evaluări
- Infection Control - Presentation TranscriptDocument9 paginiInfection Control - Presentation TranscriptDaian Anthonette PiñasÎncă nu există evaluări
- When Marketing Is StrategyDocument7 paginiWhen Marketing Is StrategyMahmudulHasanRakib100% (1)
- HomeWork 132967258274904300Document8 paginiHomeWork 132967258274904300Urvashi RaoÎncă nu există evaluări
- Reading Activity 1-Coping With Alcoholic ParentsDocument2 paginiReading Activity 1-Coping With Alcoholic ParentsG BesasÎncă nu există evaluări
- DENT Neurologic CME 2018 ProgramDocument4 paginiDENT Neurologic CME 2018 Programyos_peace86Încă nu există evaluări
- Yuracare 1078649 PDFDocument28 paginiYuracare 1078649 PDFjohnkalespiÎncă nu există evaluări
- q4 Health 10 Las Week1 and 2Document11 paginiq4 Health 10 Las Week1 and 2atthearoseÎncă nu există evaluări
- Erasmus Language Exam Writing Sample EssayDocument2 paginiErasmus Language Exam Writing Sample EssaySerdar GurbanovÎncă nu există evaluări
- Sas 15Document5 paginiSas 15Kristinelou Marie ReynaÎncă nu există evaluări
- Abnormal Psychology Overview Research ApproachesDocument52 paginiAbnormal Psychology Overview Research ApproachesBatshidi SelebogoÎncă nu există evaluări
- World Psychiatry June 2017Document112 paginiWorld Psychiatry June 2017Marco Macavilca CruzÎncă nu există evaluări
- Mediclaim 2012 Policy DocumentDocument25 paginiMediclaim 2012 Policy Documentram_341Încă nu există evaluări
- Psychodynamic Formulation American Journal of Psychiatry 144 (1987) 543-555Document9 paginiPsychodynamic Formulation American Journal of Psychiatry 144 (1987) 543-555Expandedmind100% (1)
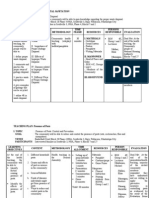
- Teaching PlanDocument16 paginiTeaching Plandeklear100% (6)
- C. Family Nursing Care Plan: Saint Louis UniversityDocument2 paginiC. Family Nursing Care Plan: Saint Louis UniversityLEONELLGABRIEL RAGUINDIN0% (1)
- Crawford - 1980 - Healthism and The Medicalization of Everyday LifeDocument24 paginiCrawford - 1980 - Healthism and The Medicalization of Everyday LifePaloma NavasÎncă nu există evaluări
- Hesi Community Health ExamDocument12 paginiHesi Community Health ExamAna BienneÎncă nu există evaluări
- The Psychology of Pain: George R. Hansen, MD, Jon Streltzer, MDDocument10 paginiThe Psychology of Pain: George R. Hansen, MD, Jon Streltzer, MDRobi Maulana100% (1)
- A Mating RelationshipDocument7 paginiA Mating RelationshipAlyanna CrisologoÎncă nu există evaluări
- Clinical Reasoning FCPDocument39 paginiClinical Reasoning FCPUlan NoputriÎncă nu există evaluări
- European Herbal Traditional Medicine Practitioners Association PDFDocument40 paginiEuropean Herbal Traditional Medicine Practitioners Association PDFNining SudrajatÎncă nu există evaluări
- Obesity Among Adults FinalDocument27 paginiObesity Among Adults Finalapi-384261910Încă nu există evaluări
- Moodule 12Document14 paginiMoodule 12camille nina jane navarroÎncă nu există evaluări
- Black S Medical Dictionary PDFDocument2.413 paginiBlack S Medical Dictionary PDFAlexandr Trotsky100% (1)
- Cross Culture Understanding: Culture Shock of IndonesiaDocument9 paginiCross Culture Understanding: Culture Shock of IndonesiaI dont knowÎncă nu există evaluări
- Coping With Diabetic Patients in Tamil Nadu-Version ReviewedDocument14 paginiCoping With Diabetic Patients in Tamil Nadu-Version Reviewedmuruga dossÎncă nu există evaluări
- A Field Manual of Camel Diseases Traditional and Modern Health Care For The DromedaryDocument273 paginiA Field Manual of Camel Diseases Traditional and Modern Health Care For The DromedaryHenrique100% (3)
- JPS-The Eleventh Meeting of The Pan Arab Gastroenterology Logy and Nutrition Society - Medics Index MembersDocument20 paginiJPS-The Eleventh Meeting of The Pan Arab Gastroenterology Logy and Nutrition Society - Medics Index MembersMedicsindex Telepin Slidecase100% (4)