S-ar putea să vă placă și
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- The Push Pull Legs RoutineDocument4 paginiThe Push Pull Legs RoutineSparkbuggy57% (7)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- Piaggio MP3 300 Ibrido LT MY 2010 (En)Document412 paginiPiaggio MP3 300 Ibrido LT MY 2010 (En)Manualles100% (3)
- Risk Management Report SummaryDocument61 paginiRisk Management Report SummaryIamCcj100% (1)
- How To Develop A Super MemoryDocument12 paginiHow To Develop A Super Memoryazik zakiÎncă nu există evaluări
- Handbook For Magnaflux L10 CoilDocument4 paginiHandbook For Magnaflux L10 CoilmgmqroÎncă nu există evaluări
- Holy Cross Academy Quarterly Cookery ExamDocument4 paginiHoly Cross Academy Quarterly Cookery ExamAlle Eiram Padillo95% (21)
- TSB 20230831 - Reconnect FATL WM Error Code & Troubleshooting GuideDocument6 paginiTSB 20230831 - Reconnect FATL WM Error Code & Troubleshooting GuideNavjot KaurÎncă nu există evaluări
- Abnegation Faction:: Clothing Is Gray and Simple. The OnlyDocument7 paginiAbnegation Faction:: Clothing Is Gray and Simple. The OnlylethaagathaÎncă nu există evaluări
- PhilLife claims process ECQDocument18 paginiPhilLife claims process ECQNoel EboniaÎncă nu există evaluări
- Chemistry CHM 1311C 2012 Test 1 BlankDocument6 paginiChemistry CHM 1311C 2012 Test 1 BlankSimon HagosÎncă nu există evaluări
- Preferensi Konsumen &strategi Pemasaran Produk Bayem Organik Di CVDocument8 paginiPreferensi Konsumen &strategi Pemasaran Produk Bayem Organik Di CVsendang mÎncă nu există evaluări
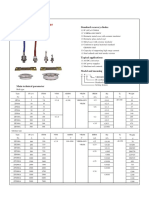
- ZP Series Silicon Rectifier: Standard Recovery DiodesDocument1 paginăZP Series Silicon Rectifier: Standard Recovery DiodesJocemar ParizziÎncă nu există evaluări
- Olpers MilkDocument4 paginiOlpers MilkARAAJ YOUSUFÎncă nu există evaluări
- CHAPTER 15 Managing Current AssetsDocument26 paginiCHAPTER 15 Managing Current AssetsAhsanÎncă nu există evaluări
- Compensation and BenefitsDocument8 paginiCompensation and BenefitsOthman FaroussiÎncă nu există evaluări
- Delta C200 Series AC Drives PDFDocument5 paginiDelta C200 Series AC Drives PDFspÎncă nu există evaluări
- Corn Pulao Recipe With Sweet CornDocument2 paginiCorn Pulao Recipe With Sweet CornSudharshanÎncă nu există evaluări
- Notes Lecture No 3 Cell Injury and MechanismDocument5 paginiNotes Lecture No 3 Cell Injury and MechanismDr-Rukhshanda RamzanÎncă nu există evaluări
- Role of Homeostasis in Human Physiology A ReviewDocument5 paginiRole of Homeostasis in Human Physiology A ReviewNathaly ZiékteÎncă nu există evaluări
- Ethnobotany Manual 14th September 2016Document54 paginiEthnobotany Manual 14th September 2016Rahul0% (1)
- Stepan Formulation 943Document2 paginiStepan Formulation 943Mohamed AdelÎncă nu există evaluări
- Limetas Maximos ResidualesDocument27 paginiLimetas Maximos ResidualesXjoelx Olaya GonzalesÎncă nu există evaluări
- Sampling & Data AssayDocument22 paginiSampling & Data AssayFerdinand SiahaanÎncă nu există evaluări
- CSK - W - My - Mother - at - Sixty - Six 2Document2 paginiCSK - W - My - Mother - at - Sixty - Six 2Aaron JoshiÎncă nu există evaluări
- Darnell's Father Goes StrictDocument2 paginiDarnell's Father Goes StrictDavid Theodore Richardson IIIÎncă nu există evaluări
- 12 2022 Salary Slip SintexDocument1 pagină12 2022 Salary Slip SintexpathyashisÎncă nu există evaluări
- Pakistan List of Approved Panel PhysicianssDocument5 paginiPakistan List of Approved Panel PhysicianssGulzar Ahmad RawnÎncă nu există evaluări
- Nursing Care of ElderlyDocument26 paginiNursing Care of ElderlyIndra KumarÎncă nu există evaluări
- QUICK CLOSING VALVE INSTALLATION GUIDEDocument22 paginiQUICK CLOSING VALVE INSTALLATION GUIDEAravindÎncă nu există evaluări
- Arecaceae or Palmaceae (Palm Family) : Reported By: Kerlyn Kaye I. AsuncionDocument23 paginiArecaceae or Palmaceae (Palm Family) : Reported By: Kerlyn Kaye I. AsuncionNamae BacalÎncă nu există evaluări