S-ar putea să vă placă și
- Cambridge Behavioural InventoryDocument4 paginiCambridge Behavioural InventoryDaniela Blanco100% (1)
- Basc-2 Presentation - All SlidesDocument59 paginiBasc-2 Presentation - All Slidesapi-290174387100% (1)
- Millon1993 PDFDocument5 paginiMillon1993 PDFSzandor X. Lecter-LaVeyÎncă nu există evaluări
- Abas 3 Chapter 5Document62 paginiAbas 3 Chapter 5GF David SalasÎncă nu există evaluări
- Schoolagecbcl PDFDocument4 paginiSchoolagecbcl PDFHeni puspitasariÎncă nu există evaluări
- NCBRF ScoreSheetDocument3 paginiNCBRF ScoreSheetPryscilla Ugas WisnarÎncă nu există evaluări
- 2013 - Cochran Autism Plus Spectrum Disorders Intersection With Psychosis and Schizophrenia Spectrum PDFDocument19 pagini2013 - Cochran Autism Plus Spectrum Disorders Intersection With Psychosis and Schizophrenia Spectrum PDFConstanza González GutiérrezÎncă nu există evaluări
- Minnesota Multiphasic Personality Inventory (MMPI-2)Document12 paginiMinnesota Multiphasic Personality Inventory (MMPI-2)Timothy JamesÎncă nu există evaluări
- Norms For An Abbreviated Raven's Coloured Progressive Matrices in An Older Sample PDFDocument11 paginiNorms For An Abbreviated Raven's Coloured Progressive Matrices in An Older Sample PDFAnonymous 7YP3VYÎncă nu există evaluări
- Estimation of Premorbid Intelligence in Spanish People With The Word Accentuation Test and Its Application To The Diagnosis of DemenciaDocument14 paginiEstimation of Premorbid Intelligence in Spanish People With The Word Accentuation Test and Its Application To The Diagnosis of DemenciathebeholderÎncă nu există evaluări
- Wisconsin Card Sorting Test Embedded Validity Indicators Developed For Adults Can Be Extended To ChildrenDocument16 paginiWisconsin Card Sorting Test Embedded Validity Indicators Developed For Adults Can Be Extended To ChildrenAnonymous 7YP3VYÎncă nu există evaluări
- 4960 4843 1 PB PDFDocument21 pagini4960 4843 1 PB PDFSartini Roma Dame NainggolanÎncă nu există evaluări
- Basic Measurement Theory: Patrick Suppes and Joseph L. ZinnesDocument134 paginiBasic Measurement Theory: Patrick Suppes and Joseph L. ZinnesYana PotÎncă nu există evaluări
- American Board of Pediatric NeuropsychologyDocument43 paginiAmerican Board of Pediatric NeuropsychologyErns Jean-baptisteÎncă nu există evaluări
- Iq and AdaptativeDocument27 paginiIq and AdaptativeRaul Morales VillegasÎncă nu există evaluări
- Adaptive Behavior Assessment System-II: Technical ReportDocument5 paginiAdaptive Behavior Assessment System-II: Technical ReportLisa MariaÎncă nu există evaluări
- The Co-Occurrence of Intellectual Giftedness and Autism Spectrum 2011Document22 paginiThe Co-Occurrence of Intellectual Giftedness and Autism Spectrum 2011Ingrid DíazÎncă nu există evaluări
- WWW - Pica.gov - JM Wp-Content Uploads 2014 06 Jamaica-Passport-Application-Compressed PDFDocument6 paginiWWW - Pica.gov - JM Wp-Content Uploads 2014 06 Jamaica-Passport-Application-Compressed PDFlorna_thomas3348Încă nu există evaluări
- Diagnosing Autism-Analyses of Data From The Autism Diagnostic Interview-CASO 3Document17 paginiDiagnosing Autism-Analyses of Data From The Autism Diagnostic Interview-CASO 3Betania MendozaÎncă nu există evaluări
- Eating Disorders InventoryDocument12 paginiEating Disorders InventoryImad SalhaÎncă nu există evaluări
- Management of Childhood and Adolescent DisordersDocument26 paginiManagement of Childhood and Adolescent Disordersdurgesh yadav100% (1)
- Psychology Project 2016-2017: The Indian Community School, KuwaitDocument21 paginiPsychology Project 2016-2017: The Indian Community School, KuwaitnadirkadhijaÎncă nu există evaluări
- Bip FLDocument2 paginiBip FLapi-460189664Încă nu există evaluări
- Lucy Barnard-Brack - Revising Social Communication Questionnaire Scoring Procedures For Autism Spectrum Disorder and Potential Social Communication DisorderDocument1 paginăLucy Barnard-Brack - Revising Social Communication Questionnaire Scoring Procedures For Autism Spectrum Disorder and Potential Social Communication DisorderAUCDÎncă nu există evaluări
- Score Sheet PsychscreenDocument2 paginiScore Sheet Psychscreenark1974Încă nu există evaluări
- Malingering and Neurological Basis of Crime: Presented by Ayesha, Fiza, Sahar, UsmaniaDocument87 paginiMalingering and Neurological Basis of Crime: Presented by Ayesha, Fiza, Sahar, UsmaniaMehroba malikÎncă nu există evaluări
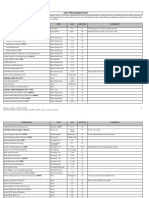
- List of Psychological TestsDocument15 paginiList of Psychological Testsnauw zÎncă nu există evaluări
- AUTISM 101: A Psychoeducational Intervention For Parents of Newly Diagnosed Children With Autism Spectrum DisorderDocument1 paginăAUTISM 101: A Psychoeducational Intervention For Parents of Newly Diagnosed Children With Autism Spectrum DisorderAUCDÎncă nu există evaluări
- Abas II Tech RPTDocument5 paginiAbas II Tech RPTUche AnekeÎncă nu există evaluări
- Adaptive Behavior Profiles in Autism Spectrum Disorders: DisclosuresDocument14 paginiAdaptive Behavior Profiles in Autism Spectrum Disorders: DisclosuresAbd El-RahmanÎncă nu există evaluări
- Age 16 Child Behavior Checklist External Site MM FinalDocument6 paginiAge 16 Child Behavior Checklist External Site MM FinalSammy FilipeÎncă nu există evaluări
- Aspergers Syndrome Through The LifespanDocument8 paginiAspergers Syndrome Through The LifespanAdnan Zaki BunyaminÎncă nu există evaluări
- Clinical Diagnosis of Alzheimer's Disease (1984, Neurology)Document8 paginiClinical Diagnosis of Alzheimer's Disease (1984, Neurology)robertokutcherÎncă nu există evaluări
- Emotional CPR - AustraliaDocument1 paginăEmotional CPR - AustraliaSharon A Stocker0% (1)
- CGASDocument4 paginiCGASDinny Atin AmanahÎncă nu există evaluări
- Abas 3 Chapter 4Document12 paginiAbas 3 Chapter 4GF David SalasÎncă nu există evaluări
- Cognitive Assessment ToolkitDocument24 paginiCognitive Assessment ToolkitTeuku Ona AriefÎncă nu există evaluări
- Bayley-III Developmental DomainsDocument4 paginiBayley-III Developmental DomainsYuri medrano100% (1)
- NPT Report DataDocument3 paginiNPT Report Datafiend007Încă nu există evaluări
- 16PF BibDocument10 pagini16PF BibdocagunsÎncă nu există evaluări
- Autism Spectrum DisorderDocument8 paginiAutism Spectrum DisorderJechsa De GuiaÎncă nu există evaluări
- Structured Group Reminiscence - An Intervention For Older AdultsDocument9 paginiStructured Group Reminiscence - An Intervention For Older AdultsDébora Ponte100% (1)
- Tom TestDocument14 paginiTom TestPaula MacielÎncă nu există evaluări
- The Ucsd Performance-Based Skills Assessment (Upsa-Brief) : Administration & Scoring ManualDocument24 paginiThe Ucsd Performance-Based Skills Assessment (Upsa-Brief) : Administration & Scoring ManualIrina StamateÎncă nu există evaluări
- NBSE Evidence-Based Review Test Summary TablesDocument82 paginiNBSE Evidence-Based Review Test Summary TablesIcaroÎncă nu există evaluări
- Autism PDFDocument41 paginiAutism PDFflower21Încă nu există evaluări
- EBP Report 2020.n PDFDocument143 paginiEBP Report 2020.n PDFcamila FuentesÎncă nu există evaluări
- Best Practices in Play Assessment and InterventionDocument12 paginiBest Practices in Play Assessment and InterventionTeresa NotoÎncă nu există evaluări
- Conners2011 PDFDocument297 paginiConners2011 PDFCristinaÎncă nu există evaluări
- Bip FLDocument5 paginiBip FLapi-460189664Încă nu există evaluări
- S3 CARS 2 SampleWriteUp 1Document1 paginăS3 CARS 2 SampleWriteUp 1Janet FernandezÎncă nu există evaluări
- Drawing Notes PDFDocument1 paginăDrawing Notes PDFM.DalaniÎncă nu există evaluări
- CV For Dr. Keely KolmesDocument9 paginiCV For Dr. Keely KolmesdrkkolmesÎncă nu există evaluări
- Guidelines For Psychological Testing of Deaf and Hard of Hearing StudentsDocument23 paginiGuidelines For Psychological Testing of Deaf and Hard of Hearing StudentsMihai Predescu100% (1)
- Shin 2006Document9 paginiShin 2006MilosÎncă nu există evaluări
- The Association Between Theory of Mind, Executive Function, and The Symptoms of Autism Spectrum DisorderDocument15 paginiThe Association Between Theory of Mind, Executive Function, and The Symptoms of Autism Spectrum DisorderRaúl VerdugoÎncă nu există evaluări
- NIMH Family Support ScaleDocument20 paginiNIMH Family Support ScaleShambhu KaratiÎncă nu există evaluări
- Advanced Interpretation of The WISCDocument4 paginiAdvanced Interpretation of The WISCCarina CamponeroÎncă nu există evaluări
- JoDD 17-1 26-37 Schroeder Et AlDocument12 paginiJoDD 17-1 26-37 Schroeder Et AlEspíritu CiudadanoÎncă nu există evaluări
- Long-Term Memory Problems in Children and Adolescents: Assessment, Intervention, and Effective InstructionDe la EverandLong-Term Memory Problems in Children and Adolescents: Assessment, Intervention, and Effective InstructionÎncă nu există evaluări
- Technical Writing - CorrespondenceDocument17 paginiTechnical Writing - CorrespondenceZaki AkramÎncă nu există evaluări
- FML File FinalDocument36 paginiFML File FinalKunal SainiÎncă nu există evaluări
- Chapter 3Document31 paginiChapter 3AntoÎncă nu există evaluări
- 6 Evaluating Community Empowerment The Purpose of Evaluation in A Programme ContextDocument32 pagini6 Evaluating Community Empowerment The Purpose of Evaluation in A Programme ContextHardiyantiÎncă nu există evaluări
- Tiffany Dewalt Assistant Principal Resume WeeblyDocument3 paginiTiffany Dewalt Assistant Principal Resume Weeblyapi-280178369Încă nu există evaluări
- K To 12 Position PaperDocument2 paginiK To 12 Position PaperCRIZZLL HANNAH MANLAVI PABILLOREÎncă nu există evaluări
- Interpersonal Communication Test 1 Study GuideDocument7 paginiInterpersonal Communication Test 1 Study GuidemothermonsterballÎncă nu există evaluări
- Classification Pros ConsDocument1 paginăClassification Pros ConsCem ErsoyÎncă nu există evaluări
- Innovating To Learn, Learn To InnovateDocument260 paginiInnovating To Learn, Learn To Innovatemacovic2Încă nu există evaluări
- WLP#28 English8 2019-2020Document4 paginiWLP#28 English8 2019-2020Anonymous FNahcfÎncă nu există evaluări
- The Principle of Politeness in The English and Uzbek LanguagesDocument6 paginiThe Principle of Politeness in The English and Uzbek Languagesaygul IsmailovaÎncă nu există evaluări
- Miftahul Janna (11614200754)Document6 paginiMiftahul Janna (11614200754)Deni AhmadÎncă nu există evaluări
- Attitudes Towards Error Correction in The Romanian ContextDocument7 paginiAttitudes Towards Error Correction in The Romanian ContexthannahÎncă nu există evaluări
- PORTFOLIO Opinion Essays ClassDocument5 paginiPORTFOLIO Opinion Essays ClassCalin Chelcea100% (1)
- 10 1111@j 1460-9568 2006 04785 X PDFDocument13 pagini10 1111@j 1460-9568 2006 04785 X PDFTlaloc GonzalezÎncă nu există evaluări
- (Zeigarnik, B.) Experimental Abnormal PsychologyDocument162 pagini(Zeigarnik, B.) Experimental Abnormal PsychologyE Alan CórdovaÎncă nu există evaluări
- Job SatisfactionDocument106 paginiJob SatisfactionShop987 ss100% (1)
- Career Guidance Seminar WorkshopDocument32 paginiCareer Guidance Seminar WorkshopRoi Khaisser Torre67% (3)
- The Danger of A Single StoryDocument3 paginiThe Danger of A Single StoryPaijen Joy Quiambao AlasÎncă nu există evaluări
- GUIDE BOOK ISIF 2020-ReducedDocument20 paginiGUIDE BOOK ISIF 2020-ReducedImamÎncă nu există evaluări
- There Is No Right or Wrong Way Exploring Expressive Dance Assignments in Physical EducationDocument15 paginiThere Is No Right or Wrong Way Exploring Expressive Dance Assignments in Physical EducationWindi SaputraÎncă nu există evaluări
- 3 Micro Project Proposal (2) ChemistryDocument2 pagini3 Micro Project Proposal (2) Chemistryashish patilÎncă nu există evaluări
- SMEPA 2020-2021: May Anne C. AlmarioDocument19 paginiSMEPA 2020-2021: May Anne C. AlmarioMay Anne Almario100% (3)
- Short Passage Lesson PlanDocument7 paginiShort Passage Lesson PlanThapanat Boon-yingÎncă nu există evaluări
- Stategic Management chp1-3Document34 paginiStategic Management chp1-3kalebÎncă nu există evaluări
- TTLG Proficiency ArgumentDocument3 paginiTTLG Proficiency Argumentapi-546255049Încă nu există evaluări
- Organizational Change and Development Chapter 12Document27 paginiOrganizational Change and Development Chapter 12Basavaraj PatilÎncă nu există evaluări
- Agro Ecosystem AnalysisDocument10 paginiAgro Ecosystem AnalysisJamil ur rahman67% (3)
- Unit 2, Lesson 1.1 - Vocab & ReadingDocument3 paginiUnit 2, Lesson 1.1 - Vocab & Readingthu thuy NguyenÎncă nu există evaluări
- Implementation of Guidance and Counseling Services During The COVID-19 PandemicDocument13 paginiImplementation of Guidance and Counseling Services During The COVID-19 PandemicAloha AntonioÎncă nu există evaluări