S-ar putea să vă placă și
- AMH Six Sigma Wait Time Project 2Document14 paginiAMH Six Sigma Wait Time Project 2maquilaconfeccionesÎncă nu există evaluări
- Egrmgmt 280 - Write-UpDocument3 paginiEgrmgmt 280 - Write-UpMackendro ChabungbamÎncă nu există evaluări
- Godwin-Regency Plaza Case StudyDocument1 paginăGodwin-Regency Plaza Case Studygiggico100% (1)
- Swot Analysis of Go AirDocument2 paginiSwot Analysis of Go Airmangesh_7735100% (1)
- POM Quiz QuestionsDocument12 paginiPOM Quiz QuestionsPrashant PanditÎncă nu există evaluări
- Case 1 - Group 8Document10 paginiCase 1 - Group 8VishvendraÎncă nu există evaluări
- Project Management-1006Document18 paginiProject Management-1006api-3776226Încă nu există evaluări
- Lecturing Note 4 Chuong 1Document55 paginiLecturing Note 4 Chuong 129. Nguyễn Thị Ý NhaÎncă nu există evaluări
- Six SigmaDocument27 paginiSix SigmaagarwalsaurabhhÎncă nu există evaluări
- Chapter 1 - Introduction To Sales MarketingDocument34 paginiChapter 1 - Introduction To Sales MarketingKhairin NorlihanÎncă nu există evaluări
- Mazda Quality Management SystemDocument6 paginiMazda Quality Management SystemHunter Frasca0% (1)
- Operations StrategyDocument26 paginiOperations Strategysulabhagarwal1985Încă nu există evaluări
- Operations Strategy PresentationDocument48 paginiOperations Strategy PresentationYannick Harvey100% (2)
- Resume 3 How To Fail in Project Management (Without Really Trying)Document6 paginiResume 3 How To Fail in Project Management (Without Really Trying)eshaeelelyeÎncă nu există evaluări
- Improvement Initiatives in GCR InsuranceDocument20 paginiImprovement Initiatives in GCR InsuranceJoe Wongkar50% (2)
- Research Methodology Hypothesis On Kia SeltosDocument2 paginiResearch Methodology Hypothesis On Kia SeltosAjitha P.NÎncă nu există evaluări
- RegencyPlaza Online Case StudyDocument8 paginiRegencyPlaza Online Case Studygal3688100% (2)
- CHP 20Document18 paginiCHP 20Mehul VadgamaÎncă nu există evaluări
- KPMG Lean Six Sigma Offerings - IIM - RanchiDocument19 paginiKPMG Lean Six Sigma Offerings - IIM - RanchiPranav Patil100% (1)
- FEIGENBAUM + Ishikawa + TaguchiDocument7 paginiFEIGENBAUM + Ishikawa + Taguchiaulia rakhmawatiÎncă nu există evaluări
- Operation MGT Practice QuestionDocument60 paginiOperation MGT Practice Questionmalik92305Încă nu există evaluări
- Teradyne Corporation - Part 1Document3 paginiTeradyne Corporation - Part 1shelzakhanÎncă nu există evaluări
- Sumeru Case SolutionDocument2 paginiSumeru Case SolutionAshwin KumarÎncă nu există evaluări
- Managerial Communication 1: Submitted ToDocument11 paginiManagerial Communication 1: Submitted TohatebookÎncă nu există evaluări
- PRM - Analyzing The Singer CaseDocument10 paginiPRM - Analyzing The Singer CasegiourtiÎncă nu există evaluări
- Aerospace Lean Six Sigma NadeemDocument4 paginiAerospace Lean Six Sigma NadeemSyedNadeemAhmedÎncă nu există evaluări
- Establishing+a+Lean+Six+Sigma+Program+in+Higher+Education+-+Author ManuscriptDocument18 paginiEstablishing+a+Lean+Six+Sigma+Program+in+Higher+Education+-+Author Manuscriptimran24Încă nu există evaluări
- 3d Robotics Disrupting The Drone MarketsDocument20 pagini3d Robotics Disrupting The Drone MarketsAries SantosoÎncă nu există evaluări
- Quiz Questions Chapter 3Document8 paginiQuiz Questions Chapter 3Darius HădăreanÎncă nu există evaluări
- Case Analysis Form - Fletcher ElectronicsDocument2 paginiCase Analysis Form - Fletcher ElectronicsAmir YousafÎncă nu există evaluări
- Beyond Valuation - Options Thinking in IT Project ManagementDocument15 paginiBeyond Valuation - Options Thinking in IT Project ManagementSmriti VohraÎncă nu există evaluări
- Time, Cost and Quality Trade-Off in Project ManagementDocument8 paginiTime, Cost and Quality Trade-Off in Project Managementapi-3707091100% (2)
- Business Statistics - Assignment December 2017 ZwOSoABguTDocument4 paginiBusiness Statistics - Assignment December 2017 ZwOSoABguTrajeev hunnyÎncă nu există evaluări
- Final PMDocument16 paginiFinal PMVijay Garg100% (1)
- Performance ManagementDocument18 paginiPerformance ManagementAkshayÎncă nu există evaluări
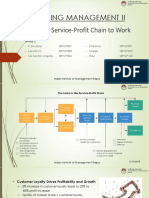
- Marketing Management Ii: Putting The Service-Profit Chain To WorkDocument10 paginiMarketing Management Ii: Putting The Service-Profit Chain To WorksrivatsavÎncă nu există evaluări
- BPR & The OrganizationDocument32 paginiBPR & The Organizationabhinav pandeyÎncă nu există evaluări
- APM Group-6 Case StudyDocument16 paginiAPM Group-6 Case StudyShikhir AgarwalÎncă nu există evaluări
- Project Management - Managing Project Uncertainty - From Variation To ChaosDocument11 paginiProject Management - Managing Project Uncertainty - From Variation To ChaosArnab Guha MallikÎncă nu există evaluări
- Design For The Next Generation: Incorporating Cradle-to-Cradle Design Into Herman Miller ProductsDocument18 paginiDesign For The Next Generation: Incorporating Cradle-to-Cradle Design Into Herman Miller ProductsJesús Rafael Páez LópezÎncă nu există evaluări
- Lean Tool Glosary - Top 25Document3 paginiLean Tool Glosary - Top 25funchesitoÎncă nu există evaluări
- Marriott Case Study PMIDocument3 paginiMarriott Case Study PMIUsama ZafarÎncă nu există evaluări
- Delivery Strategy At: Supply Chain Management (IE 659) Professor - Dr. Sanchoy K. DasDocument19 paginiDelivery Strategy At: Supply Chain Management (IE 659) Professor - Dr. Sanchoy K. DasNicolas TellezÎncă nu există evaluări
- Is This A Six Sigma, Lean, or Kaizen Project?: Terence T. BurtonDocument2 paginiIs This A Six Sigma, Lean, or Kaizen Project?: Terence T. BurtonCarlos Moreira da SilvaÎncă nu există evaluări
- Measuring Customers Perceptions-3080Document9 paginiMeasuring Customers Perceptions-3080Jagadish AppajiÎncă nu există evaluări
- Mahindra Jit Case StudyDocument2 paginiMahindra Jit Case StudySagar BhavsarÎncă nu există evaluări
- Andersen F7Document3 paginiAndersen F7Divyanshu Jain100% (1)
- Leading A Supply Chain TurnaroundDocument16 paginiLeading A Supply Chain TurnaroundSiddharth PuranikÎncă nu există evaluări
- Team Wikispeed: Developing Hardware The Software Way Please See The Questions Below and Be Prepared To Discuss in Our Next ClassDocument2 paginiTeam Wikispeed: Developing Hardware The Software Way Please See The Questions Below and Be Prepared To Discuss in Our Next ClassRAFAEL ANGELO BAUTISTAÎncă nu există evaluări
- Single Minute Exchange of Dies College ProjectDocument99 paginiSingle Minute Exchange of Dies College ProjectAkshay Shah50% (2)
- Mckinsey 7-S ModelDocument26 paginiMckinsey 7-S ModelManeesh SharmaÎncă nu există evaluări
- Six SigmaDocument35 paginiSix SigmaVeeresh Kumar RÎncă nu există evaluări
- Agile Manufacturing CaseDocument3 paginiAgile Manufacturing CaseAngela Vesleño100% (1)
- Six Sigma Project WorkDocument34 paginiSix Sigma Project WorkDrpallavi NanavatiÎncă nu există evaluări
- Quality Control: Lucila B. Rabuco, PHDDocument47 paginiQuality Control: Lucila B. Rabuco, PHDChito PermejoÎncă nu există evaluări
- V105 Article HanaffiDocument15 paginiV105 Article HanaffiCarlo SacdalanÎncă nu există evaluări
- A1 - Mini Presentation - SigmaDocument13 paginiA1 - Mini Presentation - SigmaKuljit KaurÎncă nu există evaluări
- Improving Standards of Patient Care:: Clinical AuditsDocument40 paginiImproving Standards of Patient Care:: Clinical AuditsChristina SuhadiÎncă nu există evaluări
- How To Perform Clinical AuditDocument70 paginiHow To Perform Clinical AuditFaiq Syukri Bin SaparudinÎncă nu există evaluări
- AMH Six Sigma Wait Time ProjectDocument26 paginiAMH Six Sigma Wait Time ProjectTania100% (1)
- λ-based Design Rules PDFDocument3 paginiλ-based Design Rules PDFvinosujaÎncă nu există evaluări
- Assessment of Reinforcement CorrosionDocument5 paginiAssessment of Reinforcement CorrosionClethHirenÎncă nu există evaluări
- Wireless Body Area Networks: A SurveyDocument29 paginiWireless Body Area Networks: A Surveyabdul hananÎncă nu există evaluări
- Caution!: Portable Digital Color Doppler Ultrasound SystemDocument177 paginiCaution!: Portable Digital Color Doppler Ultrasound SystemDaniel Galindo100% (1)
- C3691 - NEC, NPN Transistor, 100v, 7v Base, 5A, High Switching SpeedDocument3 paginiC3691 - NEC, NPN Transistor, 100v, 7v Base, 5A, High Switching SpeedLangllyÎncă nu există evaluări
- Rcfe Contract SSHDocument240 paginiRcfe Contract SSHJeanne MarshÎncă nu există evaluări
- 2537 - York YCAS 690Document11 pagini2537 - York YCAS 690Md JamilÎncă nu există evaluări
- DELTA - IA-HMI - Danfoss VLT 2800 - FC Protocol - CM - EN - 20111122Document4 paginiDELTA - IA-HMI - Danfoss VLT 2800 - FC Protocol - CM - EN - 20111122Ronnie Ayala SandovalÎncă nu există evaluări
- BOB SO Information HandoutDocument5 paginiBOB SO Information HandoutKabya SrivastavaÎncă nu există evaluări
- BC-5000&BC-5150 - Service Training Material - V1.0 - EN (REV)Document137 paginiBC-5000&BC-5150 - Service Training Material - V1.0 - EN (REV)iisputÎncă nu există evaluări
- High Performance HTP eDocument14 paginiHigh Performance HTP ejohnny_cashedÎncă nu există evaluări
- Curriculum Vitae: Rajeev RanjanDocument3 paginiCurriculum Vitae: Rajeev RanjanPratik AnandÎncă nu există evaluări
- Reynolds EqnDocument27 paginiReynolds EqnSuman KhanalÎncă nu există evaluări
- Studiu Privind Dezvoltarea Robotilor de Constructii Din JaponiaDocument4 paginiStudiu Privind Dezvoltarea Robotilor de Constructii Din JaponiaChelemen MaryaÎncă nu există evaluări
- Installation of Water HeatersDocument5 paginiInstallation of Water HeatersLaura KurniawanÎncă nu există evaluări
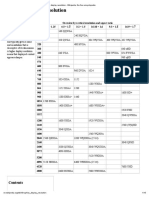
- Graphics Display Resolution - Wikipedia, The Free EncyclopediaDocument15 paginiGraphics Display Resolution - Wikipedia, The Free EncyclopediaKarun KumarÎncă nu există evaluări
- Serial NumberDocument3 paginiSerial NumberNidal Nakhalah67% (3)
- PL54 PeugeotDocument3 paginiPL54 Peugeotbump4uÎncă nu există evaluări
- Resume EeeeDocument4 paginiResume EeeeWhilmark Tican MucaÎncă nu există evaluări
- 11kv BB1Document1 pagină11kv BB1Hammadiqbal12Încă nu există evaluări
- ProductBrochure A35F A40F en 30A1006561Document24 paginiProductBrochure A35F A40F en 30A1006561Ji UvexÎncă nu există evaluări
- TPMS - A Learning GuideDocument14 paginiTPMS - A Learning GuideOrangeElectronicUsaÎncă nu există evaluări
- Metal Additive Manufacturing For Propulsion AppliDocument1 paginăMetal Additive Manufacturing For Propulsion Appliagilan89Încă nu există evaluări
- Conveni Pack Technical Data (LRYCP DY1 R 407C)Document188 paginiConveni Pack Technical Data (LRYCP DY1 R 407C)HoàngViệtAnhÎncă nu există evaluări
- Evaluasi Keandalan PLTA Bakaru: Akbar Tanjung, Arman Jaya, Suryanto, ApolloDocument8 paginiEvaluasi Keandalan PLTA Bakaru: Akbar Tanjung, Arman Jaya, Suryanto, Apollohilda tangkeÎncă nu există evaluări
- Rishabh SharmaDocument72 paginiRishabh SharmaAmitt MalhotraÎncă nu există evaluări
- 88 Numerical Series BASED TECHNOLOGY AWARENESS Grigory GRABOVOIJADocument5 pagini88 Numerical Series BASED TECHNOLOGY AWARENESS Grigory GRABOVOIJAStellaEstel93% (15)
- d350 Taper Lock End Anchor Tech Data SheetDocument2 paginid350 Taper Lock End Anchor Tech Data SheetEdsantadÎncă nu există evaluări
- Weapon Lights and Targeting LasersDocument3 paginiWeapon Lights and Targeting LasersバラモスまさゆきÎncă nu există evaluări
- Dry DockingDocument27 paginiDry DockingRoshan D'silva100% (1)