S-ar putea să vă placă și
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Schneider Pressure Switch XMLDocument2 paginiSchneider Pressure Switch XMLhaoÎncă nu există evaluări
- Column, Slab, Footing and Wall Footing Foundations: Class A MixingDocument47 paginiColumn, Slab, Footing and Wall Footing Foundations: Class A MixingGioharry Nul PanambulanÎncă nu există evaluări
- VBAC MCQsDocument3 paginiVBAC MCQsHanaÎncă nu există evaluări
- Reviews: The Global Epidemiology of HypertensionDocument15 paginiReviews: The Global Epidemiology of Hypertensionrifa iÎncă nu există evaluări
- Rail Vehicle DynamicsDocument55 paginiRail Vehicle DynamicsdfÎncă nu există evaluări
- Updated Factory Profile of Aleya Apparels LTDDocument25 paginiUpdated Factory Profile of Aleya Apparels LTDJahangir Hosen0% (1)
- Fines Reduction Project at Wendling Bowser QuarryDocument2 paginiFines Reduction Project at Wendling Bowser QuarryMarcos Antonio ParoliniÎncă nu există evaluări
- Soldier of Fortune PDFDocument208 paginiSoldier of Fortune PDFNixel SpielÎncă nu există evaluări
- JKJKJDocument3 paginiJKJKJjosecarlosvjÎncă nu există evaluări
- Irina Maleeva - Ariel Snowflake x6 - ENG - FreeDocument4 paginiIrina Maleeva - Ariel Snowflake x6 - ENG - FreeMarinaKorzinaÎncă nu există evaluări
- Industrial Artificial Intelligence For Industry 4.0-Based Manufacturing SystemsDocument5 paginiIndustrial Artificial Intelligence For Industry 4.0-Based Manufacturing SystemsMuhammad HaziqÎncă nu există evaluări
- Goldhofer FTV 850 BrochureDocument2 paginiGoldhofer FTV 850 BrochureMauroÎncă nu există evaluări
- Eng DS Epp-2314 1410Document2 paginiEng DS Epp-2314 1410MarkusAldoMaquÎncă nu există evaluări
- Board Replacement CasesDocument41 paginiBoard Replacement CasesNadeeshÎncă nu există evaluări
- Shree New Price List 2016-17Document13 paginiShree New Price List 2016-17ontimeÎncă nu există evaluări
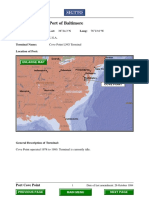
- Port Name: Port of BaltimoreDocument17 paginiPort Name: Port of Baltimoremohd1khairul1anuarÎncă nu există evaluări
- PPT DIARHEA IN CHILDRENDocument31 paginiPPT DIARHEA IN CHILDRENRifka AnisaÎncă nu există evaluări
- tGr12OM CheResoBookU78910Document110 paginitGr12OM CheResoBookU78910Jamunanantha PranavanÎncă nu există evaluări
- Stalthon Rib and InfillDocument2 paginiStalthon Rib and InfillAndrea GibsonÎncă nu există evaluări
- Electricity NotesDocument35 paginiElectricity Notesapi-277818647Încă nu există evaluări
- Electric ScootorDocument40 paginiElectric Scootor01fe19bme079Încă nu există evaluări
- Dual Shield 7100 Ultra: Typical Tensile PropertiesDocument3 paginiDual Shield 7100 Ultra: Typical Tensile PropertiesDino Paul Castro HidalgoÎncă nu există evaluări
- Owner'S Manual: 2023 Chassis CabDocument444 paginiOwner'S Manual: 2023 Chassis CabDmitry DimasÎncă nu există evaluări
- Gypsum Plasterboard: National Standard of The People'S Republic of ChinaDocument15 paginiGypsum Plasterboard: National Standard of The People'S Republic of ChinaGarry100% (2)
- L27/38S Project Guide - Power Plant: Four-Stroke GensetDocument392 paginiL27/38S Project Guide - Power Plant: Four-Stroke GensetAaron Chan100% (1)
- Ficha Tecnica-Skyjack SJ3219 8mtDocument2 paginiFicha Tecnica-Skyjack SJ3219 8mtLESLY MILENA MORENO CORALÎncă nu există evaluări
- 07ercoskun 05 01 PDFDocument23 pagini07ercoskun 05 01 PDFjagmadridÎncă nu există evaluări
- Comparing Exponential NumbersDocument5 paginiComparing Exponential NumbersMaya RahayuÎncă nu există evaluări
- Manual PipsDocument5 paginiManual PipsOzzyÎncă nu există evaluări
- Napoleonic WargamingDocument13 paginiNapoleonic WargamingandyÎncă nu există evaluări