S-ar putea să vă placă și
- The Muscle Up Guide Main PDFDocument30 paginiThe Muscle Up Guide Main PDFtano47100% (2)
- Management of Cirrhosis of The LiverDocument48 paginiManagement of Cirrhosis of The LiverksofianaÎncă nu există evaluări
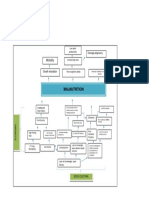
- Problem Tree Analysis MalnutritionDocument1 paginăProblem Tree Analysis MalnutritionMho Dsb50% (6)
- Pinggang Pinoy For KIDS User Invokes Fair Use Under RA8293Document13 paginiPinggang Pinoy For KIDS User Invokes Fair Use Under RA8293Rene MollenidoÎncă nu există evaluări
- Liver Cirrhosis: Review HepatologyDocument71 paginiLiver Cirrhosis: Review HepatologyAstri Arri FebriantiÎncă nu există evaluări
- Pre Test 5 QuestionsDocument12 paginiPre Test 5 QuestionsKatrina De VeraÎncă nu există evaluări
- LeanBodyChallenge ProgDocument11 paginiLeanBodyChallenge ProgMuzammil KhanÎncă nu există evaluări
- Marieb Ch3aDocument27 paginiMarieb Ch3aapi-229554503Încă nu există evaluări
- Hepatorenal Syndrome: Causes, Tests, and Treatment OptionsDe la EverandHepatorenal Syndrome: Causes, Tests, and Treatment OptionsEvaluare: 4.5 din 5 stele4.5/5 (2)
- Thesis About Monosodium GlutamateDocument33 paginiThesis About Monosodium GlutamateArrianne Jaye Mata40% (10)
- Quiz 1 - MacromoleculesDocument3 paginiQuiz 1 - MacromoleculesMariano Valiente Jr.Încă nu există evaluări
- Done By: Dana Othman: AscitesDocument28 paginiDone By: Dana Othman: Ascitesraed faisalÎncă nu există evaluări
- Cirrhosis of Liver, Liver Cancer, HepatitisDocument72 paginiCirrhosis of Liver, Liver Cancer, HepatitisBabita DhruwÎncă nu există evaluări
- Fat Burning Lasers For Surgical Body SculptingDocument5 paginiFat Burning Lasers For Surgical Body SculptingsrimatsimhasaneshwarÎncă nu există evaluări
- Boys BMI growth chart 2-20 yearsDocument1 paginăBoys BMI growth chart 2-20 yearsNisrina PuspaningarasÎncă nu există evaluări
- Chronic Kidney DiseaseDocument40 paginiChronic Kidney DiseasePaul SinsÎncă nu există evaluări
- Chronic Kidney DiseaseDocument7 paginiChronic Kidney DiseaseLardel Balbiran LafortezaÎncă nu există evaluări
- Department of Faculty SurgeryDocument40 paginiDepartment of Faculty SurgeryMandar GokhaleÎncă nu există evaluări
- Deped Order No. 13., S. 2017 "Policy and Guidelines On Healthy Food and Beverage Choices in Schools and in Deped OfficesDocument51 paginiDeped Order No. 13., S. 2017 "Policy and Guidelines On Healthy Food and Beverage Choices in Schools and in Deped OfficesAngelica GaliciaÎncă nu există evaluări
- AbdomenDocument48 paginiAbdomenAnne Marjorie Futalan100% (1)
- Chronic Liver Disease and CirrhosisDocument5 paginiChronic Liver Disease and Cirrhosisaqil ithninÎncă nu există evaluări
- Liver Cirrhosis (VD)Document56 paginiLiver Cirrhosis (VD)HannaTashiaClaudiaÎncă nu există evaluări
- The Hepatorenal SyndromeDocument26 paginiThe Hepatorenal SyndromeWaraBawanaÎncă nu există evaluări
- Pa Tho Physiology of Liver Cirrhosis - MercyDocument7 paginiPa Tho Physiology of Liver Cirrhosis - Mercymersenie_TheovercomerÎncă nu există evaluări
- Liver function tests, ultrasound, biopsy guide to interpreting resultsDocument14 paginiLiver function tests, ultrasound, biopsy guide to interpreting resultsshihochan100% (2)
- HcirhosisDocument11 paginiHcirhosisChetendra IndoliaÎncă nu există evaluări
- Sirosis Hepatis: Sigit Widyatmoko Fakultas Kedokteran UMSDocument66 paginiSirosis Hepatis: Sigit Widyatmoko Fakultas Kedokteran UMSArif Rahman DmÎncă nu există evaluări
- Chronic Liver FailureDocument4 paginiChronic Liver FailureJasmine Faith SilvaÎncă nu există evaluări
- Hepatic Cirrhosis and Hepatitis: Dr. Lubna DwerijDocument69 paginiHepatic Cirrhosis and Hepatitis: Dr. Lubna DwerijNoor MajaliÎncă nu există evaluări
- Cirrhosis of LiverDocument6 paginiCirrhosis of LiverpakdejackÎncă nu există evaluări
- Jasmin O. Dingle BSN-4y1-3CDocument6 paginiJasmin O. Dingle BSN-4y1-3CJasmn DingleÎncă nu există evaluări
- Renal SyndromeDocument13 paginiRenal SyndromeAndreas KristianÎncă nu există evaluări
- Uworld GI NotesDocument17 paginiUworld GI NotesAyodeji SotimehinÎncă nu există evaluări
- Acute Liver Failure & Hepatorenal Syndrome Diagnosis and ManagementDocument53 paginiAcute Liver Failure & Hepatorenal Syndrome Diagnosis and ManagementArnavjyoti DasÎncă nu există evaluări
- Case 36 AscitesDocument4 paginiCase 36 AscitesMichaelÎncă nu există evaluări
- AscitesDocument5 paginiAscitesEeshuAomÎncă nu există evaluări
- Fulminant Hepatic FailureDocument10 paginiFulminant Hepatic FailureAira Anne Tonee VillaminÎncă nu există evaluări
- Dr. S.P. Hewawasam (MD) Consultant Gastroenterologist/Senior Lecturer in PhysiologyDocument33 paginiDr. S.P. Hewawasam (MD) Consultant Gastroenterologist/Senior Lecturer in PhysiologyAjung SatriadiÎncă nu există evaluări
- Liver Cirrhosis: Causes, Complications and ManagementDocument55 paginiLiver Cirrhosis: Causes, Complications and ManagementAnonymous vUEDx8100% (1)
- Sirrhosis HatiDocument6 paginiSirrhosis HatikimokberusungÎncă nu există evaluări
- Cirrhosis Alcoholic Liver DiseaseDocument10 paginiCirrhosis Alcoholic Liver DiseaseSarah ZiaÎncă nu există evaluări
- Cirrhosis Complications: Causes, Symptoms, and TreatmentDocument50 paginiCirrhosis Complications: Causes, Symptoms, and Treatmentnathan asfahaÎncă nu există evaluări
- CKDDDocument11 paginiCKDDAnaÎncă nu există evaluări
- HepaticDocument5 paginiHepaticCosmin StoicaÎncă nu există evaluări
- Painless Jaundice CaseDocument8 paginiPainless Jaundice CaseStarr NewmanÎncă nu există evaluări
- The Use of Albumin For The Prevention of Hepatorenal Syndrome in Patients With Spontaneous Bacterial Peritonitis and CirrhosisDocument14 paginiThe Use of Albumin For The Prevention of Hepatorenal Syndrome in Patients With Spontaneous Bacterial Peritonitis and CirrhosisPaulus MetehÎncă nu există evaluări
- Acute Liver Failure 2012Document47 paginiAcute Liver Failure 2012nancy voraÎncă nu există evaluări
- AscitesDocument71 paginiAscitessohilaw210Încă nu există evaluări
- Role of Nurse Practitioners in The Management of Cirrhotic PatientsDocument6 paginiRole of Nurse Practitioners in The Management of Cirrhotic Patientsleti komaliaÎncă nu există evaluări
- Acute Pancreatitis: Mycobacterium Avium Complex), Peritoneal Dialysis, Cardiopulmonary Bypass, ERCPDocument8 paginiAcute Pancreatitis: Mycobacterium Avium Complex), Peritoneal Dialysis, Cardiopulmonary Bypass, ERCPRizka KartikasariÎncă nu există evaluări
- Management of End-Stage Liver DiseaseDocument34 paginiManagement of End-Stage Liver DiseaseAldo IbarraÎncă nu există evaluări
- Ontent Reviewers: Contributors:: Rishi Desai, MD, MPH Kaia Chessen Tanner Marshall, MS Will Wei Anca-Elena StefanDocument13 paginiOntent Reviewers: Contributors:: Rishi Desai, MD, MPH Kaia Chessen Tanner Marshall, MS Will Wei Anca-Elena StefanAgnes TanicÎncă nu există evaluări
- Pancreatitis: Pancreatitis Is Inflammation of The Pancreas. It Occurs When Pancreatic Enzymes (Especially Trypsin)Document6 paginiPancreatitis: Pancreatitis Is Inflammation of The Pancreas. It Occurs When Pancreatic Enzymes (Especially Trypsin)tianallyÎncă nu există evaluări
- Renal SyndromeDocument18 paginiRenal SyndromeHafshah SumayyahÎncă nu există evaluări
- Renal SyndromeDocument18 paginiRenal SyndromeRami NaifÎncă nu există evaluări
- Renal SyndromeDocument18 paginiRenal SyndromeManuel Ricardo Espinoza GutarraÎncă nu există evaluări
- Renal SyndromeDocument18 paginiRenal SyndromeRami NaifÎncă nu există evaluări
- Diagnosis and treatment of hepatorenal syndromeDocument19 paginiDiagnosis and treatment of hepatorenal syndromeOmar1895Încă nu există evaluări
- Adult Health Nursing Phase I Thursday 6:00-9:00 PM: Irritable Bowel SyndromeDocument18 paginiAdult Health Nursing Phase I Thursday 6:00-9:00 PM: Irritable Bowel SyndromeLavinia Malazarte CaballeroÎncă nu există evaluări
- College of Medicine: Thi Qar UniversityDocument30 paginiCollege of Medicine: Thi Qar Universityhussain AltaherÎncă nu există evaluări
- Gallbladder DiseaseDocument67 paginiGallbladder DiseaseKhadira MohammedÎncă nu există evaluări
- Liver Cirrhosis: Etiology Pathogenesis Clinical Features Management PrognosisDocument35 paginiLiver Cirrhosis: Etiology Pathogenesis Clinical Features Management PrognosisMohd Johari Mohd ShafuwanÎncă nu există evaluări
- JaundiceDocument3 paginiJaundiceNyaoNyao MarcellanaÎncă nu există evaluări
- Ascites: Phillip S. Ge, MD, Carlos Guarner, MD, PHD, and Bruce A. Runyon, MDDocument12 paginiAscites: Phillip S. Ge, MD, Carlos Guarner, MD, PHD, and Bruce A. Runyon, MDTere DelgadoÎncă nu există evaluări
- Cirrhosis and Hepatocellular Carcinoma GuideDocument9 paginiCirrhosis and Hepatocellular Carcinoma GuideGeorge WinchesterÎncă nu există evaluări
- CirrosisDocument44 paginiCirrosisflorilett marian cifuentesÎncă nu există evaluări
- Liver CirrhosisDocument4 paginiLiver CirrhosisromyÎncă nu există evaluări
- Chapter - 2 - C - II Liver CirrhosisDocument39 paginiChapter - 2 - C - II Liver CirrhosisEmmaÎncă nu există evaluări
- Primary Biliary CirrhosisDocument8 paginiPrimary Biliary CirrhosisAhmed TeebiÎncă nu există evaluări
- How To Work-Up A Patient With JaundiceDocument6 paginiHow To Work-Up A Patient With JaundiceTatum CheneyÎncă nu există evaluări
- Hepatorenal Syndrome - UpToDateDocument26 paginiHepatorenal Syndrome - UpToDateAssault AmphibiansÎncă nu există evaluări
- 841 Yoga SQPDocument7 pagini841 Yoga SQPShreya Singh100% (1)
- Geriatric Nutrition PresentationDocument64 paginiGeriatric Nutrition Presentationwa2nagungpÎncă nu există evaluări
- How To Spin A PencilDocument5 paginiHow To Spin A PencilJoseph JohnsonÎncă nu există evaluări
- Nafld: DR. Shatdal Chaudhary MDDocument42 paginiNafld: DR. Shatdal Chaudhary MDWaqar AhmedÎncă nu există evaluări
- Insulin GlargineDocument2 paginiInsulin GlarginePatricia MaglasangÎncă nu există evaluări
- Fitness Index TestDocument3 paginiFitness Index TestkarzinomÎncă nu există evaluări
- Unmet Needs in Hispanic/Latino Patients With Type 2 Diabetes MellitusDocument8 paginiUnmet Needs in Hispanic/Latino Patients With Type 2 Diabetes MellitusChris WilliamsÎncă nu există evaluări
- TonymatelliDocument11 paginiTonymatelliapi-326819896Încă nu există evaluări
- Day 15 Short Writing - 1Document1 paginăDay 15 Short Writing - 1Internship Reports BdÎncă nu există evaluări
- "Dyslipidemia" : Dyslipidemia Caused by Excessive Hepatic Secretion of VLDLDocument5 pagini"Dyslipidemia" : Dyslipidemia Caused by Excessive Hepatic Secretion of VLDLDANEKKA TANÎncă nu există evaluări
- Battisti Exercices PediatrieDocument197 paginiBattisti Exercices Pediatrieahkrab100% (1)
- Revisiting The Compensatory Theory As An Explanatory Model ForDocument10 paginiRevisiting The Compensatory Theory As An Explanatory Model ForDouglas RodriguesÎncă nu există evaluări
- PBL (CVS)Document2 paginiPBL (CVS)Dharshan RamÎncă nu există evaluări
- Writing Task 2Document50 paginiWriting Task 2Khanh Chi Pham100% (1)
- Guidelines HPNDocument46 paginiGuidelines HPNSherif AbobakrÎncă nu există evaluări
- Review Jurnal International Mengenai DiabetesDocument2 paginiReview Jurnal International Mengenai DiabetesRhindy Nurnaningsy SÎncă nu există evaluări
- Report, narrative and analytical exposition text featuresDocument3 paginiReport, narrative and analytical exposition text featuresVhiaLiviaÎncă nu există evaluări
- Due 6 March 2018, 9:30am Attached To Bcourses: PH150E/CP117AC: Community Health - HW Assignment #3 Spring 2018Document7 paginiDue 6 March 2018, 9:30am Attached To Bcourses: PH150E/CP117AC: Community Health - HW Assignment #3 Spring 2018Megha BanerjeeÎncă nu există evaluări