S-ar putea să vă placă și
- Intraoperative Recruitment Manoeuvres: Protective Ventilation in The ORDocument7 paginiIntraoperative Recruitment Manoeuvres: Protective Ventilation in The ORGede Eka Putra NugrahaÎncă nu există evaluări
- Hazards of Endotracheal AnaesthesiaDocument12 paginiHazards of Endotracheal AnaesthesiaGede Eka Putra NugrahaÎncă nu există evaluări
- Child-Pugh Score: Patient Name: - DateDocument3 paginiChild-Pugh Score: Patient Name: - DateGede Eka Putra NugrahaÎncă nu există evaluări
- Update On The Management of LaryngospasmDocument6 paginiUpdate On The Management of LaryngospasmGede Eka Putra NugrahaÎncă nu există evaluări
- Psoriasis - Pathophysiology, Conventional, and Alternative Approaches To TreatmentDocument24 paginiPsoriasis - Pathophysiology, Conventional, and Alternative Approaches To TreatmentGede Eka Putra NugrahaÎncă nu există evaluări
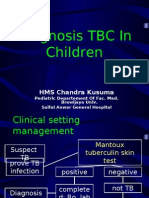
- Diagnosis TBDocument44 paginiDiagnosis TBGede Eka Putra NugrahaÎncă nu există evaluări
- Kesehatan Anak Slide Acute Renal FailureDocument21 paginiKesehatan Anak Slide Acute Renal FailureBasory Ok OkÎncă nu există evaluări
- Pathogenesis TBDocument39 paginiPathogenesis TBGede Eka Putra NugrahaÎncă nu există evaluări
- Acute Bronchitis: HMS Chandra KusumaDocument16 paginiAcute Bronchitis: HMS Chandra KusumaGede Eka Putra NugrahaÎncă nu există evaluări
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Abbreviations For O&G IndustryDocument38 paginiAbbreviations For O&G IndustryMike George MeyerÎncă nu există evaluări
- 100 IELTS Essay Topics For IELTS Writing - My IELTS Classroom BlogDocument16 pagini100 IELTS Essay Topics For IELTS Writing - My IELTS Classroom BlogtestÎncă nu există evaluări
- Tadano450xl PDFDocument12 paginiTadano450xl PDFmunawar0% (1)
- Paper 19 AugustDocument552 paginiPaper 19 AugustUma Sankar Pradhan100% (1)
- Designing The Workplace For CollaborationDocument17 paginiDesigning The Workplace For Collaborationmas zak danielÎncă nu există evaluări
- Media Analysis-GraphicDocument1 paginăMedia Analysis-Graphicapi-262266786100% (1)
- WB-Mech 120 Ch05 ModalDocument16 paginiWB-Mech 120 Ch05 ModalhebiyongÎncă nu există evaluări
- Mooka Panchsati Arya SatakamDocument18 paginiMooka Panchsati Arya SatakamPrasad Raviprolu100% (1)
- Siemens 6SL31622AA000AA0 CatalogDocument20 paginiSiemens 6SL31622AA000AA0 CatalogIrfan NurdiansyahÎncă nu există evaluări
- 2400 8560 PR 8010 - A1 HSE Management PlanDocument34 pagini2400 8560 PR 8010 - A1 HSE Management PlanMohd Musa HashimÎncă nu există evaluări
- Defining Who Is A Volunteer ConceptualDocument21 paginiDefining Who Is A Volunteer ConceptualYosep Trisaputro WahyuÎncă nu există evaluări
- DIFFERENCE BETWEEN Intrior Design and DecorationDocument13 paginiDIFFERENCE BETWEEN Intrior Design and DecorationSadaf khanÎncă nu există evaluări
- MHD Exam 6 MaterialDocument179 paginiMHD Exam 6 Materialnaexuis5467100% (1)
- PriceDoxy 09 September 2011Document56 paginiPriceDoxy 09 September 2011Elena OltuÎncă nu există evaluări
- Defining The Market Research Problem & Developing An ApproachDocument77 paginiDefining The Market Research Problem & Developing An ApproachSakshi Bhati I H21O41Încă nu există evaluări
- TSR 9294 DLA3 Dragons RestDocument78 paginiTSR 9294 DLA3 Dragons RestLéo Duarte100% (4)
- 27 Technip Energies - JD (PWD Students Only)Document1 pagină27 Technip Energies - JD (PWD Students Only)0901EE201067 KUNAL JOLLY SAXENAÎncă nu există evaluări
- Design and Fabrication of Light Electric VehicleDocument14 paginiDesign and Fabrication of Light Electric VehicleAshish NegiÎncă nu există evaluări
- Study of Noise Mapping at Moolchand Road Phargang New DelhiDocument10 paginiStudy of Noise Mapping at Moolchand Road Phargang New DelhiEditor IJTSRDÎncă nu există evaluări
- RKS IFC 2015 Solar CellDocument23 paginiRKS IFC 2015 Solar CellAnugrah PangeranÎncă nu există evaluări
- Erp FinalDocument33 paginiErp FinaltenetchatÎncă nu există evaluări
- Lesson 2.4Document8 paginiLesson 2.4Tobi TobiasÎncă nu există evaluări
- Business ProposalDocument35 paginiBusiness ProposalMJ MacapagalÎncă nu există evaluări
- Cosmology Questions and Answers - SanfoundryDocument9 paginiCosmology Questions and Answers - SanfoundryGopinathan MÎncă nu există evaluări
- An1914 PDFDocument56 paginiAn1914 PDFUpama Das100% (1)
- Tok EssayDocument2 paginiTok EssayNeto UkpongÎncă nu există evaluări
- Dawn of The DhammaDocument65 paginiDawn of The Dhammaarkaprava paulÎncă nu există evaluări
- Maxdb Backup RecoveryDocument44 paginiMaxdb Backup Recoveryft1ft1Încă nu există evaluări
- 0 - Danica Joy v. RallecaDocument2 pagini0 - Danica Joy v. RallecaRandy Jake Calizo BaluscangÎncă nu există evaluări
- Heat and Mass Chapter 2Document49 paginiHeat and Mass Chapter 2Mvelo PhungulaÎncă nu există evaluări