S-ar putea să vă placă și
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5795)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- O&G LO SlidesDocument60 paginiO&G LO Slideskatherine nunnÎncă nu există evaluări
- Management of Rectal Cancer... by DR Kassahun GirmaDocument50 paginiManagement of Rectal Cancer... by DR Kassahun GirmaKassahun Girma Gelaw100% (1)
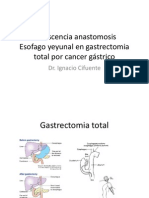
- Dehiscencia Anastomosis Esofago Yeyunal en Gastrectomia Total Por Cancer GástricoDocument22 paginiDehiscencia Anastomosis Esofago Yeyunal en Gastrectomia Total Por Cancer GástriconachooooooooÎncă nu există evaluări
- Chlamydia: Chlamydia Rapid Test Device (Swab/Urine)Document3 paginiChlamydia: Chlamydia Rapid Test Device (Swab/Urine)Cristhian CuviÎncă nu există evaluări
- ORE - UK Dental Reference BooksDocument4 paginiORE - UK Dental Reference BooksKisshore ReddyÎncă nu există evaluări
- Pediatric1 PDFDocument34 paginiPediatric1 PDFNagomi Hanison0% (1)
- Amnioinfusion - 2Document6 paginiAmnioinfusion - 2Anditha NamiraÎncă nu există evaluări
- H. Hypertensive Disorders in PregnancyDocument50 paginiH. Hypertensive Disorders in PregnancyRadha ChiombonÎncă nu există evaluări
- Screenshot 2023-11-24 at 11.55.30Document91 paginiScreenshot 2023-11-24 at 11.55.30rehab.abdel-fattahÎncă nu există evaluări
- Breastfeeding Exclusively and Iron Deficiency Anemia During The First 6 Months of AgeDocument5 paginiBreastfeeding Exclusively and Iron Deficiency Anemia During The First 6 Months of AgeDimas Fauzan TanpabasabasiÎncă nu există evaluări
- Tonsillectomy-Comparative Study of Various Techniques and Changing TrendDocument10 paginiTonsillectomy-Comparative Study of Various Techniques and Changing TrendAji Pangestu JatiÎncă nu există evaluări
- Exp 4study of Local Anesthetics by Surface Anaesthesia On The Cornea of Rabbits - LabmonkDocument5 paginiExp 4study of Local Anesthetics by Surface Anaesthesia On The Cornea of Rabbits - LabmonkSubodh ShahÎncă nu există evaluări
- Instructions For Use - IncostressDocument2 paginiInstructions For Use - IncostressGaynor MorganÎncă nu există evaluări
- Alabama Physicians LetterDocument12 paginiAlabama Physicians LetterJohn ArchibaldÎncă nu există evaluări
- Soal Un UnsratDocument80 paginiSoal Un UnsratSuzetteÎncă nu există evaluări
- Asphyxia NeonatorumDocument35 paginiAsphyxia NeonatorumMuhammad RagilÎncă nu există evaluări
- Synactive Theory of Newborn Behavioral Organization and Development - WikipediaDocument14 paginiSynactive Theory of Newborn Behavioral Organization and Development - WikipediaYuseva SariatiÎncă nu există evaluări
- 1Document25 pagini1Harvey Cj NarvasaÎncă nu există evaluări
- Effects of Implementation of Focus-Pdca Model To Decrease Patients' Length of Stay in Emergency DepartmentDocument5 paginiEffects of Implementation of Focus-Pdca Model To Decrease Patients' Length of Stay in Emergency DepartmentMuhammad RamadhanÎncă nu există evaluări
- SIBO Breath Test (Lactulose #900-C) : Z180487 For Accession #Document2 paginiSIBO Breath Test (Lactulose #900-C) : Z180487 For Accession #VICENTEÎncă nu există evaluări
- The Spirit Catches You and You Fall Down ExcerptDocument1 paginăThe Spirit Catches You and You Fall Down Excerptclim8200Încă nu există evaluări
- Anaesthesia For Cataract SurgeryDocument19 paginiAnaesthesia For Cataract SurgeryRido Banar EkaputraÎncă nu există evaluări
- Cross Section Heart - Superior Inferior Vena CavaDocument2 paginiCross Section Heart - Superior Inferior Vena CavaAlice Del Rosario CabanaÎncă nu există evaluări
- Notification SMS Medical College Jaipur SR Medical Officer PostsDocument4 paginiNotification SMS Medical College Jaipur SR Medical Officer PostsNeha SharmaÎncă nu există evaluări
- Romania Fact SheetDocument2 paginiRomania Fact SheetEmeseDengÎncă nu există evaluări
- Final Surgery RevisionDocument195 paginiFinal Surgery RevisionAbdulziz Al-jedaieÎncă nu există evaluări
- 15 - Ramos v. CA, GR No. 124354 (2002)Document4 pagini15 - Ramos v. CA, GR No. 124354 (2002)Carie LawyerrÎncă nu există evaluări
- Abigail Seidman TestimonyDocument7 paginiAbigail Seidman TestimonySpiritus_FilmsÎncă nu există evaluări
- Fetal BehaviourDocument1 paginăFetal BehaviourJuan José Espinoza OsoresÎncă nu există evaluări
- Anatomy: Patellar Tendon TearDocument11 paginiAnatomy: Patellar Tendon TearrahadianpambudiÎncă nu există evaluări