S-ar putea să vă placă și
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- NR500 W2 Scholarly Communications Worksheet-2Document4 paginiNR500 W2 Scholarly Communications Worksheet-2BSN 2014Încă nu există evaluări
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Evaluating A Website ForDocument3 paginiEvaluating A Website ForBSN 2014100% (1)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Stages of Prevention - Primer On Public Health PopulationDocument2 paginiThe Stages of Prevention - Primer On Public Health PopulationBSN 201450% (2)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Creible Paper 1Document5 paginiCreible Paper 1BSN 2014Încă nu există evaluări
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- Critical LabsDocument1 paginăCritical LabsBSN 2014Încă nu există evaluări
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- NR 500 - WK 3 Identifying Scholarly ResourcesDocument1 paginăNR 500 - WK 3 Identifying Scholarly ResourcesBSN 2014Încă nu există evaluări
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- NR500 W3 Paper-2Document5 paginiNR500 W3 Paper-2BSN 2014Încă nu există evaluări
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- DNPPDocument2 paginiDNPPBSN 2014Încă nu există evaluări
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- The Stages of Prevention - Primer On Public Health PopulationDocument2 paginiThe Stages of Prevention - Primer On Public Health PopulationBSN 201450% (2)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- BallardScore ScoresheetDocument1 paginăBallardScore ScoresheetIsabel BarradasÎncă nu există evaluări
- 6th Central Pay Commission Salary CalculatorDocument15 pagini6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Assessment Info PDFDocument1 paginăAssessment Info PDFBSN 2014Încă nu există evaluări
- 6th Central Pay Commission Salary CalculatorDocument15 pagini6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- Sample Meal Plan PDFDocument1 paginăSample Meal Plan PDFBSN 2014Încă nu există evaluări
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- Normal Vital Signs & Temp by AgeDocument1 paginăNormal Vital Signs & Temp by AgeBSN 2014Încă nu există evaluări
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
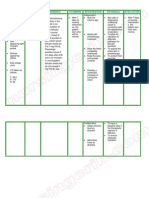
- Nursing Care Plan Hyperbilirubinemia Jaundice)Document2 paginiNursing Care Plan Hyperbilirubinemia Jaundice)deric81% (47)
- 2013 Happy Halloween Nurses Vol 2 PDFDocument19 pagini2013 Happy Halloween Nurses Vol 2 PDFBSN 2014Încă nu există evaluări
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Nurse Diagnosis PDFDocument5 paginiNurse Diagnosis PDFBSN 2014Încă nu există evaluări
- Nursing MedsDocument10 paginiNursing MedsBSN 2014Încă nu există evaluări
- An Easy Guide To Head To Toe Assessment Vrtis 12 2008 Website PDFDocument6 paginiAn Easy Guide To Head To Toe Assessment Vrtis 12 2008 Website PDFBSN 2014Încă nu există evaluări
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- An Easy Guide To Head To Toe Assessment Vrtis 12 2008 Website PDFDocument6 paginiAn Easy Guide To Head To Toe Assessment Vrtis 12 2008 Website PDFBSN 2014Încă nu există evaluări
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Erik Erikson - Psychosocial Stages - Simply PsychologyDocument5 paginiErik Erikson - Psychosocial Stages - Simply PsychologyBSN 2014Încă nu există evaluări
- SCD PathoDocument1 paginăSCD PathoBSN 2014Încă nu există evaluări
- Nursing MedsDocument10 paginiNursing MedsBSN 2014Încă nu există evaluări
- Calendarw NotesDocument12 paginiCalendarw NotesBSN 2014Încă nu există evaluări
- Respiratory Case StudyDocument2 paginiRespiratory Case StudyBSN 2014Încă nu există evaluări
- Weekly CalendarDocument1 paginăWeekly CalendarBSN 2014Încă nu există evaluări
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Careplan Acute PancreatitisDocument2 paginiCareplan Acute PancreatitisBSN 2014100% (4)
- Student Weekly Planning Calendar (Any Year, Mon-Sun) 1Document12 paginiStudent Weekly Planning Calendar (Any Year, Mon-Sun) 1ideaamulÎncă nu există evaluări
- Accu Check CompetencyDocument2 paginiAccu Check CompetencyBSN 2014Încă nu există evaluări
- COVID ProlongadoDocument22 paginiCOVID ProlongadoSMIBA MedicinaÎncă nu există evaluări
- Arterial HypertensionDocument13 paginiArterial HypertensionZedodurex100% (1)
- Medicine: Most Recent QuestionsDocument11 paginiMedicine: Most Recent QuestionsskÎncă nu există evaluări
- Hypertrophic Cardiomyopathy: Joisy Aloor Leonard Shaju Smit Bhaisare Shawn RyneDocument36 paginiHypertrophic Cardiomyopathy: Joisy Aloor Leonard Shaju Smit Bhaisare Shawn RyneJoisy Aloor100% (1)
- Chronic Inappropriate Sinus Tachycardia (Lopera)Document5 paginiChronic Inappropriate Sinus Tachycardia (Lopera)Raymond BernardusÎncă nu există evaluări
- Rubrics For Children in MurphyDocument18 paginiRubrics For Children in MurphyVirag PatilÎncă nu există evaluări
- Dilated CardiomyopathyDocument125 paginiDilated CardiomyopathyAbnet WondimuÎncă nu există evaluări
- BMI Priory Edgbaston Hospitals Consultant DirectoryDocument28 paginiBMI Priory Edgbaston Hospitals Consultant DirectorypsdsportsdocÎncă nu există evaluări
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- America Materia Medica PDFDocument470 paginiAmerica Materia Medica PDFSudhakarÎncă nu există evaluări
- How Caffeine Causes TachycardiaDocument30 paginiHow Caffeine Causes TachycardiaMadelleine PaduaÎncă nu există evaluări
- CompilationDocument41 paginiCompilationARNANTE, SOPHIA ROSE D.Încă nu există evaluări
- Heart Disease in PregnancyDocument87 paginiHeart Disease in PregnancyMonisha ArulalanÎncă nu există evaluări
- Brain Dump NUR 213 FINALDocument37 paginiBrain Dump NUR 213 FINALkelsey jackson100% (1)
- Ethnophysiology of A Khyâl AttackDocument14 paginiEthnophysiology of A Khyâl Attackdrumfiend21100% (1)
- Lee H., Kim H. A., ACN 2020, Diagnostic Approach of Orthostatic Dizziness, VertigoDocument7 paginiLee H., Kim H. A., ACN 2020, Diagnostic Approach of Orthostatic Dizziness, VertigoKeke NechÎncă nu există evaluări
- 22ND October 2017 Plab 1 MockDocument34 pagini22ND October 2017 Plab 1 MockLilim CendanaÎncă nu există evaluări
- Argentum Nitricum SCDocument7 paginiArgentum Nitricum SCnitkolÎncă nu există evaluări
- Case Scenarios University DR - NerveDocument24 paginiCase Scenarios University DR - NerveSREE NITHINÎncă nu există evaluări
- Mathew-Majus EMQ BookDocument210 paginiMathew-Majus EMQ Booksessary1Încă nu există evaluări
- Medicine MCQS JULY 2023 SOLVEDDocument15 paginiMedicine MCQS JULY 2023 SOLVEDLijo JoÎncă nu există evaluări
- Zang Fu I Heart and Small IntestineDocument43 paginiZang Fu I Heart and Small IntestineErica YangÎncă nu există evaluări
- Taiwanwalker CS Note FinalDocument50 paginiTaiwanwalker CS Note FinalNishith Labh100% (5)
- Louis Kuhne Facial Diagnosis 1897 02 PDFDocument105 paginiLouis Kuhne Facial Diagnosis 1897 02 PDFJosé BitarÎncă nu există evaluări
- 1700 Questions Not in PLABABLEDocument131 pagini1700 Questions Not in PLABABLEDaniah Marwan Dawood DAWOODÎncă nu există evaluări
- 8-Ecg in CovidsDocument35 pagini8-Ecg in CovidsyandraÎncă nu există evaluări
- 2013 ESH/ESC Practice Guidelines For The Management of Arterial HypertensionDocument14 pagini2013 ESH/ESC Practice Guidelines For The Management of Arterial HypertensionReski Melinia PatinggiÎncă nu există evaluări
- History TakingDocument13 paginiHistory TakingSirajum MuneeraÎncă nu există evaluări
- What Is Theophylline ToxicityDocument7 paginiWhat Is Theophylline ToxicitySaad BuhussainÎncă nu există evaluări
- 04 Cardiovascular TinaAbnormalsGraduateDocument3 pagini04 Cardiovascular TinaAbnormalsGraduateLMH79% (14)
- Anti Arrhythmic Drugs - FINALDocument25 paginiAnti Arrhythmic Drugs - FINALThanyun Yun100% (1)