S-ar putea să vă placă și
- Paget Disease of Bone, A Simple Guide to the Condition, Treatment and Related DiseasesDe la EverandPaget Disease of Bone, A Simple Guide to the Condition, Treatment and Related DiseasesÎncă nu există evaluări
- Gastrointestinal Anatomy and Physiology: The EssentialsDe la EverandGastrointestinal Anatomy and Physiology: The EssentialsJohn F. ReinusÎncă nu există evaluări
- Blue Boxes SummaryDocument16 paginiBlue Boxes Summaryridin007Încă nu există evaluări
- Blue Boxes For Head and NeckDocument11 paginiBlue Boxes For Head and NeckhajajyÎncă nu există evaluări
- Muscles of The Neck PDFDocument1 paginăMuscles of The Neck PDFEdreyn DellosaÎncă nu există evaluări
- Robbins Ch. 18 Liver and Biliary Tract Review QuestionsDocument12 paginiRobbins Ch. 18 Liver and Biliary Tract Review QuestionsPA2014Încă nu există evaluări
- Breasts and AxillaeDocument10 paginiBreasts and Axillaedlneisha61100% (1)
- Embryo Trans Unofficial TransDocument14 paginiEmbryo Trans Unofficial TransMark LopezÎncă nu există evaluări
- MOCK QUIZ - Head & Neck EmbryoDocument3 paginiMOCK QUIZ - Head & Neck EmbryoLanz RomuloÎncă nu există evaluări
- Anterior Compartment of Arm & Cubital FossaDocument24 paginiAnterior Compartment of Arm & Cubital FossaSky StoneÎncă nu există evaluări
- Histology of Ear and EyeDocument2 paginiHistology of Ear and EyeAnny Alvrz100% (1)
- Embryology Reviewer Chapter 1 and 2Document9 paginiEmbryology Reviewer Chapter 1 and 2Allison Eunice ServandoÎncă nu există evaluări
- 2 ThoraxDocument7 pagini2 Thoraxapi-3757921Încă nu există evaluări
- Viral Hepatitis: References: Harrisons Infectious Disease 2 Ed., Oxford Handbook of Microbiology and IdDocument58 paginiViral Hepatitis: References: Harrisons Infectious Disease 2 Ed., Oxford Handbook of Microbiology and IdMohammad Emad Al MadadhaÎncă nu există evaluări
- Physiology Summary Chapter 32Document2 paginiPhysiology Summary Chapter 32gail018Încă nu există evaluări
- Glycogen Storage Disorders PDFDocument4 paginiGlycogen Storage Disorders PDFAHMEDÎncă nu există evaluări
- Lower Limb Lab SheetDocument3 paginiLower Limb Lab SheetKelly TrainorÎncă nu există evaluări
- ANATOMY: Pelvic 2Document16 paginiANATOMY: Pelvic 2Nur Liyana MohamadÎncă nu există evaluări
- Neural Tube DefectsDocument12 paginiNeural Tube Defectsdaniel_1592Încă nu există evaluări
- Development of Branchial ArchesDocument4 paginiDevelopment of Branchial ArchesFidz Lianko100% (1)
- Human Anatomy Lecture Notes Update 2017Document58 paginiHuman Anatomy Lecture Notes Update 2017RAGHVENDRAÎncă nu există evaluări
- Surface Anatomy of HeartDocument23 paginiSurface Anatomy of HeartKhush Bakht100% (1)
- Anat - Respi Gross CompiledDocument8 paginiAnat - Respi Gross CompiledLeslie Kimberly Lisay100% (1)
- Anatomy Forum AbdDoneDocument7 paginiAnatomy Forum AbdDoneMedShare100% (1)
- TRIVIA: Dr. Tan Is The Father/Pioneer of Laparoscopic Surgery in The PhilippinesDocument48 paginiTRIVIA: Dr. Tan Is The Father/Pioneer of Laparoscopic Surgery in The PhilippinesJüdith Marie Reyes BauntoÎncă nu există evaluări
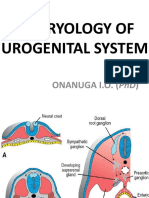
- Embryology of Urogenital SystemDocument42 paginiEmbryology of Urogenital SystemAngetile Kasanga100% (1)
- MEN1 PPDocument15 paginiMEN1 PPAaron D. PhoenixÎncă nu există evaluări
- SGDDocument7 paginiSGDJanine Vega Calayo100% (1)
- Anatomy - Pectoral Region and Axilla PDFDocument4 paginiAnatomy - Pectoral Region and Axilla PDFAngel KimÎncă nu există evaluări
- Anatomy MnemonicsDocument51 paginiAnatomy MnemonicsDrKhawarfarooq SundhuÎncă nu există evaluări
- Thyroglossal Duct CystDocument2 paginiThyroglossal Duct CystPulkitÎncă nu există evaluări
- Axillary Artery: Branches First (1 Branch) Second Part (2 Branches) Third (3 Branches) 1 2 4Document14 paginiAxillary Artery: Branches First (1 Branch) Second Part (2 Branches) Third (3 Branches) 1 2 4foster18Încă nu există evaluări
- Cardiac ExaminationDocument23 paginiCardiac ExaminationAreza Eka PermanaÎncă nu există evaluări
- Abdominal Trauma: Fatin Amirah KamaruddinDocument29 paginiAbdominal Trauma: Fatin Amirah Kamaruddinvirz23Încă nu există evaluări
- Abdominal Wall Edited WordDocument13 paginiAbdominal Wall Edited WordKennie RamirezÎncă nu există evaluări
- A Physio Midterm SGDDocument7 paginiA Physio Midterm SGDMaryÎncă nu există evaluări
- Lect 2 Descending Motor IMPROVED PathwaysDocument24 paginiLect 2 Descending Motor IMPROVED PathwaysMudassar Roomi100% (1)
- Anatomy and Physiology of Male Reproductive SystemDocument8 paginiAnatomy and Physiology of Male Reproductive SystemAdor AbuanÎncă nu există evaluări
- Pathology of Liver, Biliary, and PancreasDocument52 paginiPathology of Liver, Biliary, and PancreasHassan.shehri100% (11)
- Brainstem (Pons, Medulla, Midbrain) : Dr. MariaDocument23 paginiBrainstem (Pons, Medulla, Midbrain) : Dr. MariaMuhammad Mustaqeem100% (1)
- 1 Ana Intro Finals September 16 LaygoDocument3 pagini1 Ana Intro Finals September 16 LaygombdelenaÎncă nu există evaluări
- Gross Anatomy-Review NotesDocument56 paginiGross Anatomy-Review NotesJohnÎncă nu există evaluări
- Upper LimbDocument90 paginiUpper Limbapi-324160601100% (1)
- Obstetric Anatomy: Obstetrician & GynecologistDocument31 paginiObstetric Anatomy: Obstetrician & GynecologistnathanielÎncă nu există evaluări
- Osteology Lower Limb, by DR IramDocument76 paginiOsteology Lower Limb, by DR IramimmmiÎncă nu există evaluări
- Histology Notes 2Document13 paginiHistology Notes 2Lukas BüchlerÎncă nu există evaluări
- Renal PathDocument71 paginiRenal PathSuha AbdullahÎncă nu există evaluări
- Abdominal Cavity, Peritoneum, Abdominal EsophagusDocument4 paginiAbdominal Cavity, Peritoneum, Abdominal EsophagusMlcnd TanÎncă nu există evaluări
- Histology Practical ExamDocument7 paginiHistology Practical ExamMicky MoranteÎncă nu există evaluări
- PONS: NeuroanatomyDocument20 paginiPONS: NeuroanatomyHassan IlyasÎncă nu există evaluări
- General Principles of Gastrointestinal Motility: Alimentary TractDocument6 paginiGeneral Principles of Gastrointestinal Motility: Alimentary TractKC White Dela Rosa100% (1)
- Medical Pathology Ii. Pathology of Urinary System Lectuer NotesDocument26 paginiMedical Pathology Ii. Pathology of Urinary System Lectuer Noteseric epahÎncă nu există evaluări
- St. Luke's College of Medicine - William H. Quasha Memorial: AnatomyDocument4 paginiSt. Luke's College of Medicine - William H. Quasha Memorial: AnatomyMavic VillanuevaÎncă nu există evaluări
- Regulation RespirationDocument34 paginiRegulation Respirationkiedd_04100% (2)
- Review of Cardiovascular SystemDocument20 paginiReview of Cardiovascular SystemVăn ĐứcÎncă nu există evaluări
- Lung AbcessDocument12 paginiLung AbcessABI OFFICIALÎncă nu există evaluări
- Erb's PointDocument14 paginiErb's PointRohit SharmaÎncă nu există evaluări
- Peritoneal Anatomy Lecture NotesDocument4 paginiPeritoneal Anatomy Lecture Noteschc300Încă nu există evaluări
- A Dictionary of Human Anatomy: Skeletal SystemDe la EverandA Dictionary of Human Anatomy: Skeletal SystemÎncă nu există evaluări
- The Structure and Function of Animal Cell Components: An Introductory TextDe la EverandThe Structure and Function of Animal Cell Components: An Introductory TextÎncă nu există evaluări
- Scott - S ICMDocument29 paginiScott - S ICMkabal08Încă nu există evaluări
- PASS - Coursebook MAINDocument529 paginiPASS - Coursebook MAINkabal0850% (2)
- FisherRoulette II BookDocument68 paginiFisherRoulette II Bookkabal0850% (2)
- Dance Floor Game 101Document7 paginiDance Floor Game 101kabal08Încă nu există evaluări
- Counseling Men About SexualityDocument20 paginiCounseling Men About SexualityRicardo Garcia100% (1)
- Micromanipulation of Human Gamates and EmbryoDocument11 paginiMicromanipulation of Human Gamates and EmbryosumanavijitÎncă nu există evaluări
- Artificial Insemination of Dairy GoatsDocument2 paginiArtificial Insemination of Dairy GoatsAnthony Bonafide DakushÎncă nu există evaluări
- Assiated Reproductive Technology IpDocument25 paginiAssiated Reproductive Technology IpBharati patil100% (1)
- Androgenetic AlopeciaDocument22 paginiAndrogenetic AlopeciaYuliannisa Nyunyun100% (1)
- Dilation and CurettageDocument15 paginiDilation and Curettagenautilus81Încă nu există evaluări
- Graded RecitationDocument2 paginiGraded RecitationKath Belleza DebloisÎncă nu există evaluări
- Hipospadia, PPT Blok 3.1 (English)Document11 paginiHipospadia, PPT Blok 3.1 (English)weniÎncă nu există evaluări
- Mola Hidatidosa NcbiDocument4 paginiMola Hidatidosa NcbiRekno DwiÎncă nu există evaluări
- Maternal Taboos and The Feminine Real The Artwork of Frida Kahlo and The Matrixial Theory of Bracha L. EttingerDocument7 paginiMaternal Taboos and The Feminine Real The Artwork of Frida Kahlo and The Matrixial Theory of Bracha L. EttingerZehorith MitzÎncă nu există evaluări
- Imaging PadaDocument77 paginiImaging PadaNaja HasnandaÎncă nu există evaluări
- MCH Handbook ProjectDocument17 paginiMCH Handbook ProjectAisha MuhammadÎncă nu există evaluări
- Mary Jane Superweed Herbal Aphrodisiacs PDFDocument20 paginiMary Jane Superweed Herbal Aphrodisiacs PDFdompicnicÎncă nu există evaluări
- Mekanisme Fertilisasi PDFDocument9 paginiMekanisme Fertilisasi PDFmaulaalfarisiÎncă nu există evaluări
- MalariaDocument5 paginiMalariaRina KhazarenÎncă nu există evaluări
- Sidik-Chaula Urethroplasty and The Manset Flap For Non-Glanular Hypospadias RepairDocument8 paginiSidik-Chaula Urethroplasty and The Manset Flap For Non-Glanular Hypospadias RepairShandy JonnerÎncă nu există evaluări
- Certificate of Death 1Document2 paginiCertificate of Death 1Charley Labicani BurigsayÎncă nu există evaluări
- Different Systems of BodyDocument16 paginiDifferent Systems of BodygracetingÎncă nu există evaluări
- SN Zones States Lgas Wards Name - of - Facility - VisitedDocument33 paginiSN Zones States Lgas Wards Name - of - Facility - VisitedSalihu MustaphaÎncă nu există evaluări
- AntepartalDocument27 paginiAntepartalaliehso100% (1)
- Fish Anatomy For Fish BreedingDocument2 paginiFish Anatomy For Fish BreedinghumanupgradeÎncă nu există evaluări
- Who Labour Care GuideDocument1 paginăWho Labour Care Guidezeus balagtasÎncă nu există evaluări
- Janat00454 0079Document23 paginiJanat00454 0079BattleAppleÎncă nu există evaluări
- Orientation 2172016Document62 paginiOrientation 2172016Devi Ramadani100% (1)
- Early Pregnancy Intervention Program: City Youth Development OfficeDocument3 paginiEarly Pregnancy Intervention Program: City Youth Development OfficeSamantha sheeranÎncă nu există evaluări
- Drawing A Family Pedigree Independent Learning Module:: D - V M S, D P, G E @Document5 paginiDrawing A Family Pedigree Independent Learning Module:: D - V M S, D P, G E @Rey PinedaÎncă nu există evaluări
- 5-10 - Grasshopper - Dissection AsDocument7 pagini5-10 - Grasshopper - Dissection AsAbir OmarÎncă nu există evaluări
- List of Semen StationsDocument6 paginiList of Semen StationsYogesh NÎncă nu există evaluări
- Secondary AmenorrheaDocument18 paginiSecondary AmenorrheaMaria Gill100% (1)
- VIA (Visual Inspection With Acetic Acid Aplication) Preparation of StepsDocument20 paginiVIA (Visual Inspection With Acetic Acid Aplication) Preparation of StepsIndonesian Journal of Cancer100% (1)