S-ar putea să vă placă și
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Fax Cover Sheet: 3. Copy of Ambulance Driver License/Passport/Visa/: TEHSEEN Abbas ThomasDocument1 paginăFax Cover Sheet: 3. Copy of Ambulance Driver License/Passport/Visa/: TEHSEEN Abbas Thomasemman_abzÎncă nu există evaluări
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Ambulance Car Pass Application FormDocument1 paginăAmbulance Car Pass Application Formemman_abzÎncă nu există evaluări
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Page 1 of 2: Attach Picture HereDocument2 paginiPage 1 of 2: Attach Picture Hereemman_abzÎncă nu există evaluări
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Chemical Indicator Types Available in The CSH and Tag Identification InformationDocument4 paginiChemical Indicator Types Available in The CSH and Tag Identification Informationemman_abzÎncă nu există evaluări
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- Airborne Precaution: يبلسلا ءاوهلا طغض تحت يبطلا لزعلا ةيعضو يف ضيرم دجوي Negative Pressure Room is a mustDocument2 paginiAirborne Precaution: يبلسلا ءاوهلا طغض تحت يبطلا لزعلا ةيعضو يف ضيرم دجوي Negative Pressure Room is a mustemman_abzÎncă nu există evaluări
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Ambulance Car Pass Application FormDocument1 paginăAmbulance Car Pass Application Formemman_abzÎncă nu există evaluări
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Template For GuidelinesDocument2 paginiTemplate For Guidelinesemman_abzÎncă nu există evaluări
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Employment Contract With English Translation Original Employer Certificate of IncomeDocument1 paginăEmployment Contract With English Translation Original Employer Certificate of Incomeemman_abzÎncă nu există evaluări
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Protective Precaution: يبطلا لزعلا تحت ضيرم دجوي Isolation Room is a mustDocument2 paginiProtective Precaution: يبطلا لزعلا تحت ضيرم دجوي Isolation Room is a mustemman_abzÎncă nu există evaluări
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Mrs. Celina Conol, RN, MANDocument1 paginăMrs. Celina Conol, RN, MANemman_abzÎncă nu există evaluări
- Prayer Never Known To FailDocument1 paginăPrayer Never Known To Failemman_abzÎncă nu există evaluări
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- رشابملا لاصتصلا قيرط نع ىودعلا نم هيامحلا Contact PrecautionDocument3 paginiرشابملا لاصتصلا قيرط نع ىودعلا نم هيامحلا Contact Precautionemman_abzÎncă nu există evaluări
- Airborne Precaution: يبلسلا ءاوهلا طغض تحت يبطلا لزعلا ةيعضو يف ضيرم دجوي Negative Pressure Room is a mustDocument2 paginiAirborne Precaution: يبلسلا ءاوهلا طغض تحت يبطلا لزعلا ةيعضو يف ضيرم دجوي Negative Pressure Room is a mustemman_abzÎncă nu există evaluări
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- Top 10 Traits Every Nurse Should HaveDocument13 paginiTop 10 Traits Every Nurse Should Haveemman_abzÎncă nu există evaluări
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- What Is Heart Failure?Document2 paginiWhat Is Heart Failure?emman_abzÎncă nu există evaluări
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- How To Handle Station 2Document11 paginiHow To Handle Station 2emman_abzÎncă nu există evaluări
- Kristylle Marie N. Abelardo BS Psychology II SPSS Act: CorrelationDocument3 paginiKristylle Marie N. Abelardo BS Psychology II SPSS Act: Correlationemman_abzÎncă nu există evaluări
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Cardiac Medications by at A GlanceDocument4 paginiCardiac Medications by at A GlanceZhukma BogeeÎncă nu există evaluări
- StreptokinaseDocument8 paginiStreptokinaseemman_abzÎncă nu există evaluări
- Psych Stat Chap 5Document2 paginiPsych Stat Chap 5emman_abzÎncă nu există evaluări
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Sign and Symptoms of Coronary-SyndromeDocument11 paginiSign and Symptoms of Coronary-SyndromeRatna Pusvita Effendy'sÎncă nu există evaluări
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Ucm 300338Document2 paginiUcm 300338julia007Încă nu există evaluări
- Patient Procedures SurgeriesDocument4 paginiPatient Procedures SurgeriesTracyÎncă nu există evaluări
- What Is Coronary Angiography?Document4 paginiWhat Is Coronary Angiography?emman_abzÎncă nu există evaluări
- Eccentric Song ListDocument3 paginiEccentric Song Listemman_abzÎncă nu există evaluări
- Renal Failure Nursing Care PlanDocument2 paginiRenal Failure Nursing Care Planemman_abz33% (3)
- eDocument13 paginieemman_abzÎncă nu există evaluări
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
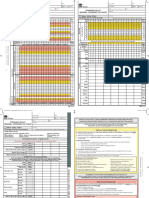
- Sample Observation Proformas: Adult Observation Chart Separate Explanatory PageDocument8 paginiSample Observation Proformas: Adult Observation Chart Separate Explanatory Pageemman_abzÎncă nu există evaluări
- Dengue Fever Nursing Care Plan-High Risk For Fluid Volume DeficitDocument1 paginăDengue Fever Nursing Care Plan-High Risk For Fluid Volume Deficitemman_abz100% (5)
- Nursing Physical AssessmentDocument2 paginiNursing Physical Assessmentemman_abzÎncă nu există evaluări
- PSMID COVID 19 Interim Guidelines v.03262020Document41 paginiPSMID COVID 19 Interim Guidelines v.03262020Athan Antonio100% (1)
- (Intubate!) : Stag e Description GFR (Ml/min/1.73Document7 pagini(Intubate!) : Stag e Description GFR (Ml/min/1.73Jamie PalmeriÎncă nu există evaluări
- Flyer Konker Pdpi 2023 23082023Document30 paginiFlyer Konker Pdpi 2023 23082023suci mesaÎncă nu există evaluări
- Management of Advanced Peritonitis PP TDocument106 paginiManagement of Advanced Peritonitis PP Tvedant kanadeÎncă nu există evaluări
- Can Postoperative Nutrition Be Favourably Maintained by Oral Diet in Patients With Emergency Temporary Ileostomy? A Tertiary Hospital Based StudyDocument5 paginiCan Postoperative Nutrition Be Favourably Maintained by Oral Diet in Patients With Emergency Temporary Ileostomy? A Tertiary Hospital Based StudydwirizqillahÎncă nu există evaluări
- Syok SepticDocument15 paginiSyok SepticJennifer GraceÎncă nu există evaluări
- Court County Death: Minnesota Hennepin GeegndjudicialDocument10 paginiCourt County Death: Minnesota Hennepin GeegndjudicialGoMNÎncă nu există evaluări
- SAGO AdultObsDocument2 paginiSAGO AdultObsTim BrownÎncă nu există evaluări
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Use of Vasopressors and Inotropes - UpToDateDocument25 paginiUse of Vasopressors and Inotropes - UpToDateVictor Mendoza - MendezÎncă nu există evaluări
- Intestinal Failure AdultsDocument12 paginiIntestinal Failure Adultssilvio da costa guerreiroÎncă nu există evaluări
- Pews Charts 4 11 MonthsDocument2 paginiPews Charts 4 11 MonthsKiara RevalinaÎncă nu există evaluări
- Fluid Balance Emma BoxallDocument13 paginiFluid Balance Emma BoxallRendra Syani Ulya FitriÎncă nu există evaluări
- Intensive Management of Pediatric Acute Liver FailureDocument11 paginiIntensive Management of Pediatric Acute Liver FailureAditya SeptiadinataÎncă nu există evaluări
- Optimizing Red Blood Cell Transfusion Practice: S. D. Surgenor, M. Hampers, and H. L. CorwinDocument10 paginiOptimizing Red Blood Cell Transfusion Practice: S. D. Surgenor, M. Hampers, and H. L. CorwinnadaÎncă nu există evaluări
- Clinical ExemplarDocument5 paginiClinical Exemplarapi-283481267Încă nu există evaluări
- The Role of The Gut Microbiota in SepsisDocument9 paginiThe Role of The Gut Microbiota in SepsisSyahrul HamidÎncă nu există evaluări
- Evaluation and Management of Suspected Sepsis and Septic Shock in Adults - UpToDateDocument37 paginiEvaluation and Management of Suspected Sepsis and Septic Shock in Adults - UpToDatebarcanbiancaÎncă nu există evaluări
- Indications and Hemoglobin Thresholds For Red Blood Cell Transfusion in The Adult - UpToDateDocument39 paginiIndications and Hemoglobin Thresholds For Red Blood Cell Transfusion in The Adult - UpToDateAhmed MostafaÎncă nu există evaluări
- Lit 2. Sepsis-3 Abdul Hakeem Al Hashim, MD, FRCPCDocument76 paginiLit 2. Sepsis-3 Abdul Hakeem Al Hashim, MD, FRCPCKomang_JananuragaÎncă nu există evaluări
- Septic ArtritisDocument41 paginiSeptic ArtritisAdit Wendy YR100% (1)
- Abdominal Compartment SyndromeDocument24 paginiAbdominal Compartment SyndromePrateek Vaswani100% (1)
- 4 5780579467025976939Document843 pagini4 5780579467025976939osama hosniÎncă nu există evaluări
- Source Control in Emergency General SurgeryDocument21 paginiSource Control in Emergency General SurgerylaviniaÎncă nu există evaluări
- Puerperal SepsisDocument11 paginiPuerperal SepsisLana LocoÎncă nu există evaluări
- Neonatal SepsisDocument8 paginiNeonatal Sepsis+nellaÎncă nu există evaluări
- Management of Miscarriage and Sepsis: EsmoeDocument29 paginiManagement of Miscarriage and Sepsis: EsmoeLana LocoÎncă nu există evaluări
- Recommended Antibiotic Therapy in Severe Sepsis or Septic ShockDocument4 paginiRecommended Antibiotic Therapy in Severe Sepsis or Septic ShockBoy ReynaldiÎncă nu există evaluări
- SepsisDocument11 paginiSepsisLisana Azkia ZaiyanÎncă nu există evaluări
- Malaria Case Studies Only - EnglishDocument11 paginiMalaria Case Studies Only - EnglishFeik Emelje100% (1)
- War Surgery - Working With Limited ResourcesDocument357 paginiWar Surgery - Working With Limited ResourcesMichael Yoder100% (1)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedDe la EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedEvaluare: 5 din 5 stele5/5 (81)
- The Obesity Code: Unlocking the Secrets of Weight LossDe la EverandThe Obesity Code: Unlocking the Secrets of Weight LossEvaluare: 4 din 5 stele4/5 (6)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDDe la EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDEvaluare: 5 din 5 stele5/5 (1)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeDe la EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeEvaluare: 2 din 5 stele2/5 (1)
- The Age of Magical Overthinking: Notes on Modern IrrationalityDe la EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityEvaluare: 4 din 5 stele4/5 (26)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionDe la EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionEvaluare: 4 din 5 stele4/5 (404)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisDe la EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisEvaluare: 4.5 din 5 stele4.5/5 (42)