S-ar putea să vă placă și
- Jurnal Inggris PDFDocument4 paginiJurnal Inggris PDFTom PrasÎncă nu există evaluări
- An Infectious Disease of Skin MCQsDocument111 paginiAn Infectious Disease of Skin MCQsDr.Tawheed67% (6)
- Syndromic Management of Sexually Transmitted InfectionsDocument76 paginiSyndromic Management of Sexually Transmitted Infectionsnamita100% (2)
- Chancroid PPT - For Class PresentationDocument12 paginiChancroid PPT - For Class PresentationBikash Sah0% (1)
- Spontaneous Vaginal Delivery IN Post Term PregnancyDocument55 paginiSpontaneous Vaginal Delivery IN Post Term Pregnancyr.pavinvikneshÎncă nu există evaluări
- Menstrual DisordersDocument29 paginiMenstrual DisorderstuhinsinghÎncă nu există evaluări
- Menstrual Disorder and Abnormal BleedingDocument9 paginiMenstrual Disorder and Abnormal Bleedingdr_asalehÎncă nu există evaluări
- Anatomy of Female Genital Tract by Sidra IftikharDocument33 paginiAnatomy of Female Genital Tract by Sidra IftikharWaqas Tahir100% (1)
- Ectopic Pregnancy (Autosaved)Document56 paginiEctopic Pregnancy (Autosaved)susmita shresthaÎncă nu există evaluări
- Benign Disease of The UterusDocument27 paginiBenign Disease of The UterusnyangaraÎncă nu există evaluări
- Electro Surgery in Gynaecology: Dept. of OBGYN M.K.C.G.Medical College Berhampur, Orissa, IndiaDocument38 paginiElectro Surgery in Gynaecology: Dept. of OBGYN M.K.C.G.Medical College Berhampur, Orissa, IndiaHossamaldin Hussein Kamel SalemÎncă nu există evaluări
- Fertilisasi Askeb IDocument19 paginiFertilisasi Askeb IPutry Utami0% (1)
- Benign Lesions of Vulva and VaginaDocument34 paginiBenign Lesions of Vulva and VaginaCabdiÎncă nu există evaluări
- Ob - Operative ObstetricsDocument224 paginiOb - Operative Obstetricsapi-385605133% (3)
- Male InfertilityDocument57 paginiMale InfertilityUsha AnengaÎncă nu există evaluări
- Abnormal Uterine Bleeding: - Rou'a Eyad - Rahaf EyadDocument35 paginiAbnormal Uterine Bleeding: - Rou'a Eyad - Rahaf EyadYazeed Asrawi0% (1)
- Menstrual Disorders: Olufemi Aworinde Lecturer/ Consultant Obstetrician and Gynaecologist, Bowen University, IwoDocument36 paginiMenstrual Disorders: Olufemi Aworinde Lecturer/ Consultant Obstetrician and Gynaecologist, Bowen University, IwoAkinbani MoyosoreÎncă nu există evaluări
- Abnormal Vaginal BleedingDocument41 paginiAbnormal Vaginal BleedingmarkkerwinÎncă nu există evaluări
- Hormonal ContraceptivesDocument25 paginiHormonal Contraceptivesmd easarur rahmanÎncă nu există evaluări
- Infections of Female Genital TractDocument67 paginiInfections of Female Genital TractSana AftabÎncă nu există evaluări
- Ectopic Pregnancy: by Amielia Mazwa Rafidah Obstetric and Gynecology DepartmentDocument43 paginiEctopic Pregnancy: by Amielia Mazwa Rafidah Obstetric and Gynecology DepartmentAlrick AsentistaÎncă nu există evaluări
- Abnormal Uterine Bleeding (AUB)Document45 paginiAbnormal Uterine Bleeding (AUB)asdf0% (1)
- Genital FistulaeDocument15 paginiGenital Fistulaesangeetha francisÎncă nu există evaluări
- PA Genitalia WanitaDocument100 paginiPA Genitalia WanitaBÎncă nu există evaluări
- Final PresentationDocument62 paginiFinal PresentationMacabio Zeil Love100% (1)
- Abnormal Uterine BleedingDocument39 paginiAbnormal Uterine BleedingVincentiusÎncă nu există evaluări
- Uterine FibroidsDocument21 paginiUterine FibroidsPrasun BiswasÎncă nu există evaluări
- (Gyne) 2.1 PCOS, Hyperandrogenism & Hyperprolactenemia (OnaCruz) - WiniDocument10 pagini(Gyne) 2.1 PCOS, Hyperandrogenism & Hyperprolactenemia (OnaCruz) - WiniDexter IanÎncă nu există evaluări
- Pulmonary Disorders in PregnancyDocument49 paginiPulmonary Disorders in PregnancyMara Medina - BorleoÎncă nu există evaluări
- Congenital Anomelies of Reproductive OrgansDocument47 paginiCongenital Anomelies of Reproductive Organsdr_shamimrÎncă nu există evaluări
- Impey Obs and Gynae Revision Notes PDFDocument9 paginiImpey Obs and Gynae Revision Notes PDFRoiseÎncă nu există evaluări
- Malignant Diseases of The CervixDocument128 paginiMalignant Diseases of The Cervixnicewan0% (1)
- Presentation 2Document49 paginiPresentation 2Wahyu Adhitya Prawirasatra100% (2)
- Infertility: Reshmi SibyDocument80 paginiInfertility: Reshmi SibySusan ThomasÎncă nu există evaluări
- Monday PresentationsDocument20 paginiMonday PresentationsSunaina BhartiÎncă nu există evaluări
- Infertility IDocument36 paginiInfertility Idr_asaleh100% (1)
- Sakila MurmuDocument47 paginiSakila MurmuSakila murmuÎncă nu există evaluări
- Women Health Presentation (Ovarian Cyst)Document17 paginiWomen Health Presentation (Ovarian Cyst)Lim Su-WeiÎncă nu există evaluări
- Pap Smear Guidelines: Baylor College of Medicine Anoop Agrawal, M.DDocument22 paginiPap Smear Guidelines: Baylor College of Medicine Anoop Agrawal, M.Dshygirl72Încă nu există evaluări
- Simposium 1 - Controversies - Dr. Teguh - HPV Vaccine Vs HPV Test-1Document20 paginiSimposium 1 - Controversies - Dr. Teguh - HPV Vaccine Vs HPV Test-1isnayu drÎncă nu există evaluări
- PDFDocument8 paginiPDFSaumya SharmaÎncă nu există evaluări
- Abnormal Uterine Bleeding: District 1 ACOG Medical Student Education Module 2008Document17 paginiAbnormal Uterine Bleeding: District 1 ACOG Medical Student Education Module 2008ninachayank0% (1)
- Uterinefibroids 130120064643 Phpapp02Document73 paginiUterinefibroids 130120064643 Phpapp02Tharun KumarÎncă nu există evaluări
- Obstetric Anal Sphincter Injury (OASIS) - UpToDateDocument39 paginiObstetric Anal Sphincter Injury (OASIS) - UpToDateErickÎncă nu există evaluări
- Cervical Intraepithelial Neoplasia and Cervical CancerDocument28 paginiCervical Intraepithelial Neoplasia and Cervical CancerNatnael100% (1)
- Laparoscopic Gynecologist Surgeon in HSR Layout BangaloreDocument8 paginiLaparoscopic Gynecologist Surgeon in HSR Layout BangaloreDr.Beena JeysinghÎncă nu există evaluări
- Lesi Pra Kanker ServiksDocument34 paginiLesi Pra Kanker ServiksNeni SetyoÎncă nu există evaluări
- Dr. Sharda Jain: Director: Secretary GeneralDocument91 paginiDr. Sharda Jain: Director: Secretary GeneraljijaniÎncă nu există evaluări
- ALARMER Dystocia PDFDocument5 paginiALARMER Dystocia PDFwilliamÎncă nu există evaluări
- Thrombocytopenia in PregnancyDocument31 paginiThrombocytopenia in Pregnancyari naÎncă nu există evaluări
- Identification and Management of Ambiguous GenitaliaDocument31 paginiIdentification and Management of Ambiguous Genitaliateslimolakunleraji100% (1)
- Management of Abnormal Pap Smears PresentationDocument17 paginiManagement of Abnormal Pap Smears Presentationapi-210786702100% (1)
- Sexually Transmitted DiseasesDocument14 paginiSexually Transmitted DiseasesMartha P0% (1)
- Polycystic Ovarian Syndrome: Dr. PrabhavathiDocument30 paginiPolycystic Ovarian Syndrome: Dr. PrabhavathiKasi PrasadÎncă nu există evaluări
- Cardiac Disease in PregnancyDocument28 paginiCardiac Disease in PregnancyviharadewiÎncă nu există evaluări
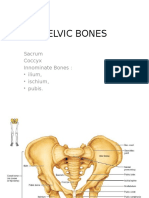
- Pelvic BoneDocument15 paginiPelvic BoneYoanneveline TanakÎncă nu există evaluări
- Menopause Dan KlimakteriumDocument20 paginiMenopause Dan KlimakteriumAlfix AnugrahÎncă nu există evaluări
- Ruptured Ectopic Pregnancy: by Lingga Lilianie Nur Safqi Guidance Dr. Reno YovialDocument31 paginiRuptured Ectopic Pregnancy: by Lingga Lilianie Nur Safqi Guidance Dr. Reno YoviallinggasafqiÎncă nu există evaluări
- Claire Maevelle A. Laxamana BSP - 3ADocument10 paginiClaire Maevelle A. Laxamana BSP - 3ACLaire Maevelle Angeles LaxamanaÎncă nu există evaluări
- Pelvic AnatomyDocument106 paginiPelvic AnatomyRosu George100% (1)
- Hydrosalpinx MBDocument30 paginiHydrosalpinx MBverhaniÎncă nu există evaluări
- Handbook of Current and Novel Protocols for the Treatment of InfertilityDe la EverandHandbook of Current and Novel Protocols for the Treatment of InfertilityMichael H. DahanÎncă nu există evaluări
- Abortion and Sterilization: Medical and Social AspectsDe la EverandAbortion and Sterilization: Medical and Social AspectsJane E. HodgsonÎncă nu există evaluări
- PlantersDocument20 paginiPlantersDanna BongonÎncă nu există evaluări
- BONGON - Alvarez v. RamirezDocument2 paginiBONGON - Alvarez v. RamirezDanna BongonÎncă nu există evaluări
- Criminal Law 2008Document9 paginiCriminal Law 2008Danna BongonÎncă nu există evaluări
- Statcon GSIS V CA DigestDocument5 paginiStatcon GSIS V CA DigestDanna BongonÎncă nu există evaluări
- Crim Law 1993Document2 paginiCrim Law 1993Danna BongonÎncă nu există evaluări
- 2 BONGON People v. AbelleraDocument2 pagini2 BONGON People v. AbelleraDanna BongonÎncă nu există evaluări
- Ethics DigestDocument25 paginiEthics DigestFersal AlbercaÎncă nu există evaluări
- Lecture 1 IntroductionDocument27 paginiLecture 1 IntroductionDanna BongonÎncă nu există evaluări
- 72 - BONGON - Great Pacific V CADocument2 pagini72 - BONGON - Great Pacific V CADanna BongonÎncă nu există evaluări
- Republic v. CapoteDocument2 paginiRepublic v. CapoteDanna BongonÎncă nu există evaluări
- Leviton Industries VDocument1 paginăLeviton Industries VDanna BongonÎncă nu există evaluări
- DR Saurabh Jindal DVT Dermatology 2020Document101 paginiDR Saurabh Jindal DVT Dermatology 2020mayurdadhaniyaÎncă nu există evaluări
- The History of Venereal Disease and Parangi in Sri LankaDocument6 paginiThe History of Venereal Disease and Parangi in Sri LankaMindStilledÎncă nu există evaluări
- Ulcer Genitalis EllenoDocument2 paginiUlcer Genitalis EllenoGabriela Sabatini GunawanÎncă nu există evaluări
- Full RujiraLeukorrhea, STDS, HIV Infection.02102017 PDFDocument129 paginiFull RujiraLeukorrhea, STDS, HIV Infection.02102017 PDFrujiraÎncă nu există evaluări
- Genital Tract Infections - GynecologyDocument17 paginiGenital Tract Infections - GynecologyKC Dela RosaÎncă nu există evaluări
- T & D - DERMATOLOGY - 2022 - QuestionDocument6 paginiT & D - DERMATOLOGY - 2022 - QuestionVyserionÎncă nu există evaluări
- Syphilis and ChancroidDocument16 paginiSyphilis and Chancroidram krishnaÎncă nu există evaluări
- Sexually Transmitted DiseasesDocument76 paginiSexually Transmitted Diseasessomaya abdulhakimÎncă nu există evaluări
- Andrews Diseases of The Skin Clinical Dermatology, 12th Ed - James, Berger, Elston, & Neuhaus - LTDocument2 paginiAndrews Diseases of The Skin Clinical Dermatology, 12th Ed - James, Berger, Elston, & Neuhaus - LTsyed rokunujjamanÎncă nu există evaluări
- EtsDocument31 paginiEtsTony Gomez Luna LeyvaÎncă nu există evaluări
- Haemophilus SPPDocument109 paginiHaemophilus SPPJamie CañebaÎncă nu există evaluări
- WHO - Guidelines For The Management of STI - 2021Document216 paginiWHO - Guidelines For The Management of STI - 2021Evivana Sri SundariÎncă nu există evaluări
- GYNE 2.01a Lower Genital Tract Infections PDFDocument12 paginiGYNE 2.01a Lower Genital Tract Infections PDFMiguel Domingo100% (1)
- Parvobacteria: Dr. Shehab Ahmed LafiDocument61 paginiParvobacteria: Dr. Shehab Ahmed Lafiقدامه زين العابدين حسان عثمانÎncă nu există evaluări
- MCQ Dermatology (Dr. Asaf K.)Document31 paginiMCQ Dermatology (Dr. Asaf K.)Dinesh JadhavÎncă nu există evaluări
- ChancroidDocument6 paginiChancroidSukmasari TÎncă nu există evaluări
- Michele Topic 5Document32 paginiMichele Topic 5MICHELE ANGELA HEREBESIÎncă nu există evaluări
- Session9-Gynecologic InfectionsDocument81 paginiSession9-Gynecologic InfectionsCHALIE MEQUÎncă nu există evaluări
- Sexually Transmitted Infections Basics in DiagnosisDocument95 paginiSexually Transmitted Infections Basics in Diagnosistummalapalli venkateswara raoÎncă nu există evaluări
- Bordetella: Bordetella Organisms Are Small, Gram-Negative Coccobacilli Which Are Strict Aerobes. The ThreeDocument7 paginiBordetella: Bordetella Organisms Are Small, Gram-Negative Coccobacilli Which Are Strict Aerobes. The ThreeFlor OMÎncă nu există evaluări
- Chancroid & Haemophilus DucreyiDocument19 paginiChancroid & Haemophilus DucreyiLalan HolalaÎncă nu există evaluări
- P2 MICRO RATIOaDocument18 paginiP2 MICRO RATIOaJemuel DalanaÎncă nu există evaluări
- Flowcharts For Management of STI-FinalDocument22 paginiFlowcharts For Management of STI-FinalJay PaulÎncă nu există evaluări
- Understanding The Self Module 2 Lesson 1Document18 paginiUnderstanding The Self Module 2 Lesson 1Marites MancerasÎncă nu există evaluări
- Etas MCQ 2015..2Document605 paginiEtas MCQ 2015..2sajithaÎncă nu există evaluări
- Gynecologic Infections: Genet Gebremedhin (MD) Assistant Prof of Gynecology & Obstetrics University of Gondar March 4 2012Document91 paginiGynecologic Infections: Genet Gebremedhin (MD) Assistant Prof of Gynecology & Obstetrics University of Gondar March 4 2012Degefaw BikoyÎncă nu există evaluări
- Sexually Transmitted Diseases in MalesDocument15 paginiSexually Transmitted Diseases in MalesSam Raven AndresÎncă nu există evaluări