S-ar putea să vă placă și
- Come To The MusicDocument13 paginiCome To The Musicdoctorwho69Încă nu există evaluări
- My Fair Lady ScriptDocument132 paginiMy Fair Lady ScriptEdwin ChaoÎncă nu există evaluări
- Sinhal ADocument13 paginiSinhal Adoctorwho69Încă nu există evaluări
- You LL Be Back Sheet Music Hamilton (The Musical) (SheetMusic Free - Com)Document8 paginiYou LL Be Back Sheet Music Hamilton (The Musical) (SheetMusic Free - Com)Heza11100% (1)
- RS Best Grunge Albums Ever PDFDocument12 paginiRS Best Grunge Albums Ever PDFdoctorwho69Încă nu există evaluări
- Gizmo Building Instructions V2p0Document86 paginiGizmo Building Instructions V2p0doctorwho69Încă nu există evaluări
- Eye MD IaDocument37 paginiEye MD Iadoctorwho69Încă nu există evaluări
- 14 Day Rapid Fat LossDocument112 pagini14 Day Rapid Fat Lossdoctorwho69100% (3)
- Gizmo Building InstructionsDocument58 paginiGizmo Building Instructionsdoctorwho69Încă nu există evaluări
- Anaesthesia For Obstructive Airway DiseaseDocument40 paginiAnaesthesia For Obstructive Airway Diseasedoctorwho69Încă nu există evaluări
- RS Best Grunge Albums EverDocument12 paginiRS Best Grunge Albums Everdoctorwho69Încă nu există evaluări
- Basic Science For AnaesthetistsDocument224 paginiBasic Science For AnaesthetistsciccioÎncă nu există evaluări
- ENT & Dental Anaesthesia 2Document22 paginiENT & Dental Anaesthesia 2doctorwho69Încă nu există evaluări
- Anesthesia in The District HospitalDocument162 paginiAnesthesia in The District HospitalPrayudi Aji MurtoloÎncă nu există evaluări
- Time Capsule Setup GuideDocument44 paginiTime Capsule Setup Guidedoctorwho69Încă nu există evaluări
- Time Capsule Setup GuideDocument44 paginiTime Capsule Setup Guidedoctorwho69Încă nu există evaluări
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Leoline Installation and MaintenanceDocument8 paginiLeoline Installation and MaintenanceFloorkitÎncă nu există evaluări
- Adobeconstruct 19 NeubDocument34 paginiAdobeconstruct 19 NeublailanuitÎncă nu există evaluări
- PW6101 ProgrammationDocument44 paginiPW6101 ProgrammationCédric DekeyserÎncă nu există evaluări
- Water Distiller - ManualDocument2 paginiWater Distiller - ManualSanjeevi JagadishÎncă nu există evaluări
- 01 Head and Neck JMDocument16 pagini01 Head and Neck JMJowi SalÎncă nu există evaluări
- The Jewish Way in Death and MourningDocument67 paginiThe Jewish Way in Death and Mourningizzy212100% (1)
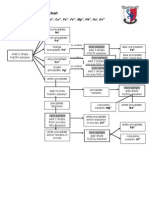
- Testing For Cations Flow ChartDocument2 paginiTesting For Cations Flow Chartapi-252561013Încă nu există evaluări
- Sensus 143-80 Service Regulator R-1301 R5Document11 paginiSensus 143-80 Service Regulator R-1301 R5Paolita Auza BalderramaÎncă nu există evaluări
- Lead and Manage People TTLMDocument41 paginiLead and Manage People TTLMHenok Mehari100% (1)
- Entomotherapy, or The Medicinal Use of InsectsDocument23 paginiEntomotherapy, or The Medicinal Use of InsectsJessica Revelo OrdoñezÎncă nu există evaluări
- Supplementary Spec To API Specification 17D Subsea Wellhead and Tree Equipment With Justifications S 561Jv2022 11Document81 paginiSupplementary Spec To API Specification 17D Subsea Wellhead and Tree Equipment With Justifications S 561Jv2022 11maximusala83Încă nu există evaluări
- hw410 Unit 9 Assignment 1Document8 paginihw410 Unit 9 Assignment 1api-600248850Încă nu există evaluări
- Polycystic Ovary Syndrome (PCOS) - Symptoms, Causes, and TreatmentDocument19 paginiPolycystic Ovary Syndrome (PCOS) - Symptoms, Causes, and TreatmentAkshay HarekarÎncă nu există evaluări
- Heat Transfer Lab AssignmentDocument5 paginiHeat Transfer Lab AssignmentChristyÎncă nu există evaluări
- Human Sociobiology: A Holistic Approach (Dan Freedman)Document126 paginiHuman Sociobiology: A Holistic Approach (Dan Freedman)Cynthia AndrewsÎncă nu există evaluări
- Rotating Driver S Workstation and Rotating Cab: Reliable Solutions For More Ergonomic and Effective WorkingDocument12 paginiRotating Driver S Workstation and Rotating Cab: Reliable Solutions For More Ergonomic and Effective WorkingEduardo CapeletiÎncă nu există evaluări
- LPG PropertiesDocument2 paginiLPG Propertiesvvk557Încă nu există evaluări
- 200mm 250mm 300 MM: Project Name Location Bill No. - 00 (Rev. 0) Consultant Contractor Buildiong Name DATEDocument2 pagini200mm 250mm 300 MM: Project Name Location Bill No. - 00 (Rev. 0) Consultant Contractor Buildiong Name DATEganesh gundÎncă nu există evaluări
- English 1 Reading (CVC)Document27 paginiEnglish 1 Reading (CVC)Angelica ArcangelÎncă nu există evaluări
- Tibia Bone Segmentation in X-Ray Images - A Comparative AnalysisDocument8 paginiTibia Bone Segmentation in X-Ray Images - A Comparative AnalysisSuzanaPetrovicÎncă nu există evaluări
- Big BazaarDocument6 paginiBig BazaaraniketsangodcarÎncă nu există evaluări
- The Bitter Internal Drive of AppleDocument7 paginiThe Bitter Internal Drive of AppleBon WambuaÎncă nu există evaluări
- Buddhist 083011Document150 paginiBuddhist 083011Mazzy S100% (1)
- Soil ExplorationDocument42 paginiSoil ExplorationDilipKumarAkkaladevi100% (1)
- Surveys For Maint'Ce ClassDocument7 paginiSurveys For Maint'Ce ClassSuhe EndraÎncă nu există evaluări
- D8045-16 Standard Test Method For Acid Number of Crude Oils and Petroleum Products by CatalyticDocument6 paginiD8045-16 Standard Test Method For Acid Number of Crude Oils and Petroleum Products by CatalytichishamÎncă nu există evaluări
- Single Conductor 15KV, Shielded, MV-105Document2 paginiSingle Conductor 15KV, Shielded, MV-105henry hernandezÎncă nu există evaluări
- Clinical Algorithms in General Surgery PDFDocument786 paginiClinical Algorithms in General Surgery PDFLaura Campaña100% (5)
- MAUS Catalogue PDFDocument10 paginiMAUS Catalogue PDFCarolina Garcés MoralesÎncă nu există evaluări
- Lesson 3.3 Inside An AtomDocument42 paginiLesson 3.3 Inside An AtomReign CallosÎncă nu există evaluări