S-ar putea să vă placă și
- Case Presentation 1Document27 paginiCase Presentation 1Inatul Aulia67% (6)
- 02 Preoperative Assessment of A Patient With Cataract-FinalDocument10 pagini02 Preoperative Assessment of A Patient With Cataract-Finalmdshahidalam315Încă nu există evaluări
- Clinical Management Review 2023-2024: Volume 2: USMLE Step 3 and COMLEX-USA Level 3De la EverandClinical Management Review 2023-2024: Volume 2: USMLE Step 3 and COMLEX-USA Level 3Încă nu există evaluări
- Case Study On GlaucomaDocument6 paginiCase Study On GlaucomaKing GamerÎncă nu există evaluări
- New ProposalDocument29 paginiNew ProposalBless CoÎncă nu există evaluări
- Pre and Post Op Cataract EvaluaDocument56 paginiPre and Post Op Cataract Evaluahenok birukÎncă nu există evaluări
- AOA Lasik Co-Management GuideDocument22 paginiAOA Lasik Co-Management GuideJitander DudeeÎncă nu există evaluări
- Guideline of Glaucoma PDFDocument30 paginiGuideline of Glaucoma PDFYunita Eka Putri DunggaÎncă nu există evaluări
- 5 Cataract-200605111818Document55 pagini5 Cataract-200605111818Ashok TawadeÎncă nu există evaluări
- Glaucoma 191024141130Document25 paginiGlaucoma 191024141130Broz100% (1)
- Chapter 11 Eye & Vision DisordersDocument72 paginiChapter 11 Eye & Vision DisordersMYLENE GRACE ELARCOSAÎncă nu există evaluări
- Cataract SurgeryDocument14 paginiCataract SurgeryRenato AbellaÎncă nu există evaluări
- Glaucoma and CataractDocument30 paginiGlaucoma and CataractJayselle ArvieÎncă nu există evaluări
- GlaucomaDocument3 paginiGlaucomaPuviyarasiÎncă nu există evaluări
- VI (Visual ImpairmentDocument24 paginiVI (Visual ImpairmentSanishka NiroshanÎncă nu există evaluări
- Management of GlaucomaDocument7 paginiManagement of GlaucomaAlbertus Bayu KristiantoÎncă nu există evaluări
- New Management Strategies For Ectopia LentisDocument14 paginiNew Management Strategies For Ectopia LentisximoÎncă nu există evaluări
- Holy 3Document3 paginiHoly 3Holy Fitria ArianiÎncă nu există evaluări
- Diabetic Eye DiseaseDocument3 paginiDiabetic Eye DiseaseRabiu Hassan MusaÎncă nu există evaluări
- 35 Golden Eye RulesDocument7 pagini35 Golden Eye RulesJethro WuÎncă nu există evaluări
- Indirect&dilationDocument9 paginiIndirect&dilationHenok BirukÎncă nu există evaluări
- 1 - MyopiaDocument9 pagini1 - MyopiaSpislgal PhilipÎncă nu există evaluări
- PT EduDocument4 paginiPT EduTasissa AyelaÎncă nu există evaluări
- PT EduDocument4 paginiPT EduTasissa AyelaÎncă nu există evaluări
- Glaucoma & Retinal Detachment-1Document29 paginiGlaucoma & Retinal Detachment-1Priya bhattiÎncă nu există evaluări
- Retinitis PigmentosaDocument45 paginiRetinitis PigmentosaANDREW OMAKAÎncă nu există evaluări
- Glaucoma: Diska Astarini I11109083Document49 paginiGlaucoma: Diska Astarini I11109083Nauli PanjaitanÎncă nu există evaluări
- Glaucoma New Zealand - A Charitable TrustDocument49 paginiGlaucoma New Zealand - A Charitable TrustMiazan SheikhÎncă nu există evaluări
- Ico Guidelines For Diabetic Eye CareDocument19 paginiIco Guidelines For Diabetic Eye CareMuhammad Usman Salim100% (1)
- Summary of The Alberta Clinical Practice Guideline, August 1996Document2 paginiSummary of The Alberta Clinical Practice Guideline, August 1996malathiÎncă nu există evaluări
- Vitrectomy Results in Proliferative Diabetic RetinopathyDocument3 paginiVitrectomy Results in Proliferative Diabetic RetinopathyRohamonangan TheresiaÎncă nu există evaluări
- AmblyopiaDocument28 paginiAmblyopiaAndhika YogiswaraÎncă nu există evaluări
- EyedisorderDocument91 paginiEyedisorderLaurensia MassariÎncă nu există evaluări
- Therapeutic Effectiveness of Toric Implantable Collamer Lens in Treating Ultrahigh Myopic AstigmatismDocument7 paginiTherapeutic Effectiveness of Toric Implantable Collamer Lens in Treating Ultrahigh Myopic AstigmatismStephanie PfengÎncă nu există evaluări
- Anaesthesia For Vitreo-Retinal SurgeryDocument6 paginiAnaesthesia For Vitreo-Retinal SurgeryRuwan KuruppuÎncă nu există evaluări
- Cataract Surgery ProtocolsDocument17 paginiCataract Surgery ProtocolsRahul ShastriÎncă nu există evaluări
- Disturbance in Sensory PerceptionDocument48 paginiDisturbance in Sensory PerceptionKristine Louise JavierÎncă nu există evaluări
- GlaucomaDocument42 paginiGlaucomaMaryTanÎncă nu există evaluări
- Cataract: Presented By: HomipalDocument12 paginiCataract: Presented By: Homipalankita singhÎncă nu există evaluări
- Anaesthesia RCOphth GuidelinesDocument4 paginiAnaesthesia RCOphth GuidelinesDiana SmithÎncă nu există evaluări
- Lasik 1 PDFDocument3 paginiLasik 1 PDFJulie JohnsonÎncă nu există evaluări
- NCM 116: Care of Clients With Problems in Nutrition and Gastrointestinal, Metabolism and Endocrine,, Acute and ChronicDocument18 paginiNCM 116: Care of Clients With Problems in Nutrition and Gastrointestinal, Metabolism and Endocrine,, Acute and ChronicDiego DumauaÎncă nu există evaluări
- Presentación Edema Macular DiabéticoDocument26 paginiPresentación Edema Macular Diabéticomauricio bayramÎncă nu există evaluări
- Diabetic RetinopathyDocument48 paginiDiabetic RetinopathyOmar HamwiÎncă nu există evaluări
- 6 GlaucomaDocument52 pagini6 GlaucomacreativejoburgÎncă nu există evaluări
- Glaukoma Dan HipermetropiDocument6 paginiGlaukoma Dan HipermetropifuadaffanÎncă nu există evaluări
- Acuity Optics Journal Articles - ParaphrasingDocument6 paginiAcuity Optics Journal Articles - ParaphrasingSyed Faisal HarmonyÎncă nu există evaluări
- Op Thom OlogyDocument88 paginiOp Thom OlogyFareed KhanÎncă nu există evaluări
- COMPLICATIONS of CATARACT SURGERY (Capsular Opacification and Contraction and Hemorrhage)Document30 paginiCOMPLICATIONS of CATARACT SURGERY (Capsular Opacification and Contraction and Hemorrhage)Hikban Fiqhi100% (1)
- Lasik GuidelinesDocument4 paginiLasik GuidelinesIlmiahdmobgyn MaretmeiÎncă nu există evaluări
- RCOphth Recruitment A4 BookletDocument12 paginiRCOphth Recruitment A4 BookletIbnu RizaÎncă nu există evaluări
- Section 6&7Document5 paginiSection 6&7kadek gita dwi anggrainiÎncă nu există evaluări
- CataractDocument38 paginiCataractruhulcoc1Încă nu există evaluări
- Ablasio RetinaDocument23 paginiAblasio RetinaResa PutraÎncă nu există evaluări
- Visual Outcome After Phacomorphic GlaucomaDocument3 paginiVisual Outcome After Phacomorphic GlaucomaHassan KhanÎncă nu există evaluări
- Rop AaoDocument29 paginiRop AaoSania NadianisaÎncă nu există evaluări
- Cataract Retinopathy Child Hood Iris Abnormalities Ocular Tumors Visual Dysfunction (Document41 paginiCataract Retinopathy Child Hood Iris Abnormalities Ocular Tumors Visual Dysfunction (Henok BirukÎncă nu există evaluări
- CD 6 OphthalmologyDocument7 paginiCD 6 OphthalmologyؤيؤييسيÎncă nu există evaluări
- Eye in Facial ParalysisDocument8 paginiEye in Facial Paralysisjoal510Încă nu există evaluări
- Eye Problems On ExpeditionsDocument7 paginiEye Problems On ExpeditionsjustanothergunnutÎncă nu există evaluări
- Kag Rully (B.IG)Document7 paginiKag Rully (B.IG)Rully Dwi SaputraÎncă nu există evaluări
- HistoryDocument9 paginiHistoryRara Aulia IIÎncă nu există evaluări
- Non-Surgical Management of SquintDocument16 paginiNon-Surgical Management of SquintAnumeha Jindal100% (2)
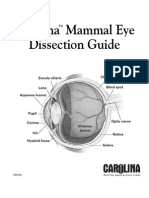
- Mammal Eye DissectionDocument4 paginiMammal Eye Dissectionnongnong2516Încă nu există evaluări
- 1 s2.0 S1367048418310452 MainDocument6 pagini1 s2.0 S1367048418310452 MainskocabzzÎncă nu există evaluări
- 130-044 EnglishDocument6 pagini130-044 EnglishMuhammad Syauqie AssegafÎncă nu există evaluări
- @@downloadDocument1 pagină@@downloadKetut AryawanÎncă nu există evaluări
- Clinical Profile of Patients of Panophthalmitis Presenting To The Tertiary Health Care CentreDocument6 paginiClinical Profile of Patients of Panophthalmitis Presenting To The Tertiary Health Care CentreIJAR JOURNALÎncă nu există evaluări
- Phacoemulsification Steps: Pande Made GustianaDocument34 paginiPhacoemulsification Steps: Pande Made GustianaPande GustianaÎncă nu există evaluări
- The Art of Medical Management in Glaucoma PDFDocument29 paginiThe Art of Medical Management in Glaucoma PDFCahyaÎncă nu există evaluări
- Red Eye Differential DiagnosisDocument70 paginiRed Eye Differential DiagnosisAdetz HaedetzÎncă nu există evaluări
- Anatomy and Physiology of EyelidDocument34 paginiAnatomy and Physiology of Eyelidsushma shrestha100% (1)
- Effect of High Add Power, Medium Add Power, or Single-VisionDocument10 paginiEffect of High Add Power, Medium Add Power, or Single-VisionAkira MasumiÎncă nu există evaluări
- Jurnal Penelitian DR EkoDocument1 paginăJurnal Penelitian DR EkoEko WidayantoÎncă nu există evaluări
- Ophthalmologic Approach To Chemical Burns - Background, Pathophysiology, EpidemiologyDocument6 paginiOphthalmologic Approach To Chemical Burns - Background, Pathophysiology, EpidemiologyAnonymous S0MyRHÎncă nu există evaluări
- Katherine E. Paton Honored As 2018 Professional of The Year in Ocular OncologyDocument2 paginiKatherine E. Paton Honored As 2018 Professional of The Year in Ocular OncologyPR.comÎncă nu există evaluări
- Most Common Ophthalmic Diagnoses in Eye Emergency Departments: A Multicenter StudyDocument8 paginiMost Common Ophthalmic Diagnoses in Eye Emergency Departments: A Multicenter StudyAlba García MarcoÎncă nu există evaluări
- Common Ophthalmic Eye DropsDocument13 paginiCommon Ophthalmic Eye DropsYew JoanneÎncă nu există evaluări
- Prakriya Hospitals Investor Brochure - 2019Document19 paginiPrakriya Hospitals Investor Brochure - 2019Abhishek S AatreyaÎncă nu există evaluări
- Macular Function TestDocument2 paginiMacular Function TestNeha SinghÎncă nu există evaluări
- Corneal Edema Post Cataract SurgeryDocument13 paginiCorneal Edema Post Cataract SurgeryPrathibha M ChachadiÎncă nu există evaluări
- Eye QuizDocument8 paginiEye QuizagwadeÎncă nu există evaluări
- Accuracy of Referral and Phone-Triage Diagnoses in An Eye Emergency DepartmentDocument3 paginiAccuracy of Referral and Phone-Triage Diagnoses in An Eye Emergency DepartmentBima RizkiÎncă nu există evaluări
- Index 9Document3 paginiIndex 9Lucas HoldereggerÎncă nu există evaluări
- Use of Dyes in OphthalmologyDocument4 paginiUse of Dyes in OphthalmologyMaulana MalikÎncă nu există evaluări
- Coding Poli Mata: Papillitis H46 Hypertension Ocular:h40.0 Macula H35.8 Ptosis H02.4 Chalazion H00.1 Asthenopia H53.1Document1 paginăCoding Poli Mata: Papillitis H46 Hypertension Ocular:h40.0 Macula H35.8 Ptosis H02.4 Chalazion H00.1 Asthenopia H53.1nurcasanÎncă nu există evaluări
- Physics of The EyeDocument59 paginiPhysics of The EyePrincess Dianna SulitÎncă nu există evaluări
- ConjunctivitisDocument9 paginiConjunctivitisSaranya DeviÎncă nu există evaluări
- Axa Group Corporate PresentationDocument35 paginiAxa Group Corporate PresentationRajneesh VermaÎncă nu există evaluări
- Human Eye: General PropertiesDocument10 paginiHuman Eye: General PropertiesVijay RajendiranÎncă nu există evaluări