S-ar putea să vă placă și
- Practice Reflection Worksheet Jithesh VKDocument3 paginiPractice Reflection Worksheet Jithesh VKapi-353376334100% (2)
- Root Cause AnalysisDocument28 paginiRoot Cause Analysisaftabseven2Încă nu există evaluări
- Erik Satie PDFDocument368 paginiErik Satie PDFarturimagem100% (2)
- Root Cause Analysis (RCA)Document153 paginiRoot Cause Analysis (RCA)Solha89% (9)
- Root Cause Analysis PresentationDocument37 paginiRoot Cause Analysis PresentationucheonixÎncă nu există evaluări
- Kaizen Event Project Charter: Project Name Agency/Division/ Location Scope Meeting Date Target Event DateDocument3 paginiKaizen Event Project Charter: Project Name Agency/Division/ Location Scope Meeting Date Target Event DateDebashishDolonÎncă nu există evaluări
- Inident Investigation Root Cause AnalysisDocument61 paginiInident Investigation Root Cause Analysisbaaziz2015Încă nu există evaluări
- Apollo Root Cause AnalysisDocument20 paginiApollo Root Cause AnalysisMohd Fakhruddin Basar100% (2)
- The Impact of Social Media Volume and Addiction On Medical StudentsDocument12 paginiThe Impact of Social Media Volume and Addiction On Medical StudentsIan Kristopher Bayan100% (1)
- Root Cause AnalysisDocument12 paginiRoot Cause Analysisosalp internationalÎncă nu există evaluări
- Risk Management Using Failure Mode and Effect Analysis (FMEA)De la EverandRisk Management Using Failure Mode and Effect Analysis (FMEA)Încă nu există evaluări
- Cause and Effect Diagram: CA/PA-RCA: Basic ToolDocument21 paginiCause and Effect Diagram: CA/PA-RCA: Basic ToolYashini BhuguthÎncă nu există evaluări
- Chapter 9. Failure Root Cause PreventionDocument23 paginiChapter 9. Failure Root Cause PreventionAbdirahman Ali mohamudÎncă nu există evaluări
- FMEADocument5 paginiFMEAmz007Încă nu există evaluări
- RCA TrainingDocument15 paginiRCA TrainingfelicityÎncă nu există evaluări
- Root Cause AnalysisDocument21 paginiRoot Cause Analysischngan432257% (7)
- Iso22000 2005Document48 paginiIso22000 2005STELLA MARISÎncă nu există evaluări
- Root Cause Analysis ReportDocument39 paginiRoot Cause Analysis ReportAliyana ShresthaÎncă nu există evaluări
- Lean Maintenance RoadmapDocument11 paginiLean Maintenance Roadmapreynancs0% (1)
- Powerful New Ideas: in Material Handling and MovementDocument9 paginiPowerful New Ideas: in Material Handling and MovementAmarjeet RaiÎncă nu există evaluări
- 10 Best Software Tools To Conduct Root Cause Analysis and Solve Complex ProblemsDocument4 pagini10 Best Software Tools To Conduct Root Cause Analysis and Solve Complex ProblemssaospieÎncă nu există evaluări
- Reliability Centered MaintenanceDocument103 paginiReliability Centered Maintenancecnrk777Încă nu există evaluări
- Plant Safety ChecklistDocument19 paginiPlant Safety ChecklistAbhishek PalÎncă nu există evaluări
- 5 Why FormDocument1 pagină5 Why Formvandukul100% (1)
- Root Causes AnalisysDocument33 paginiRoot Causes Analisysandrés_donossoÎncă nu există evaluări
- CRE Preliminary Test (30) : ASQ CRE (Certified Reliability Engineer)Document8 paginiCRE Preliminary Test (30) : ASQ CRE (Certified Reliability Engineer)Idris AbiolaÎncă nu există evaluări
- Machine Guard ChecklistDocument7 paginiMachine Guard Checklisthi2lathaÎncă nu există evaluări
- Distance Traveled by Each Paperplane Per TrialDocument13 paginiDistance Traveled by Each Paperplane Per TrialAnonymous d6EtxrtbÎncă nu există evaluări
- Quality ImprovementDocument125 paginiQuality ImprovementNia SinghÎncă nu există evaluări
- The Following Slides Are Not Contractual in Nature and Are For Information Purposes Only As of June 2015Document44 paginiThe Following Slides Are Not Contractual in Nature and Are For Information Purposes Only As of June 2015khldHA100% (1)
- RCA Report SampleDocument7 paginiRCA Report SampleErc Nunez VÎncă nu există evaluări
- Fish Bone AnalysisDocument21 paginiFish Bone AnalysisDeeksha RainaÎncă nu există evaluări
- Proact Rca TemplateDocument1 paginăProact Rca Templatetristanmaharaj100% (1)
- Root Cause TemplateDocument19 paginiRoot Cause TemplateFiroz Khan100% (3)
- Initial Stages of EvolutionDocument5 paginiInitial Stages of EvolutionVivek MulchandaniÎncă nu există evaluări
- Accident CausationDocument45 paginiAccident Causationrealneil_1100% (1)
- Document Review ChecklistDocument7 paginiDocument Review ChecklistSahabat Ceria SakmadyoneÎncă nu există evaluări
- Root cause analysis tool A Complete Guide - 2019 EditionDe la EverandRoot cause analysis tool A Complete Guide - 2019 EditionÎncă nu există evaluări
- Maintenance Data AnalysisDocument15 paginiMaintenance Data AnalysisRaju Ramaswami100% (1)
- Loto ModuleDocument34 paginiLoto Modulearturilli100% (2)
- CRE: ASQ Certified Reliability Engineer - Full: Question ResultsDocument60 paginiCRE: ASQ Certified Reliability Engineer - Full: Question ResultssskiitbÎncă nu există evaluări
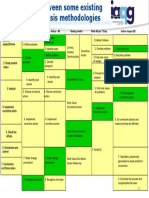
- Root Cause Analysis Methodologies IAQGDocument1 paginăRoot Cause Analysis Methodologies IAQGAldo100% (1)
- Root Cause Analysis Template 44Document3 paginiRoot Cause Analysis Template 44Devi ChintyaÎncă nu există evaluări
- Root Cause AnalysisDocument1 paginăRoot Cause AnalysisSick LoveÎncă nu există evaluări
- Control ChartsDocument19 paginiControl ChartsMichelle GoÎncă nu există evaluări
- Root Cause AnalysisDocument105 paginiRoot Cause AnalysisPunjabi Stars Update100% (1)
- Failure Mode and Effects Analysis (FMEA)Document37 paginiFailure Mode and Effects Analysis (FMEA)Charlie Tubaon100% (3)
- A3 Problem Solving Training Course OutlineDocument1 paginăA3 Problem Solving Training Course OutlineNedra DebbechÎncă nu există evaluări
- The Sinking of The Titanic Cause MapDocument6 paginiThe Sinking of The Titanic Cause MapJoseph MiladÎncă nu există evaluări
- Conducting RCAs PDFDocument4 paginiConducting RCAs PDFShariq AfridiÎncă nu există evaluări
- RCA2 ImprovingRootCauseAnalysesandActionstoPreventHarmDocument51 paginiRCA2 ImprovingRootCauseAnalysesandActionstoPreventHarmalejandromfunes1749Încă nu există evaluări
- DOE RCFA Guideline Document PDFDocument69 paginiDOE RCFA Guideline Document PDFrosyidnurdinfauziÎncă nu există evaluări
- Hazard IdentificationDocument24 paginiHazard IdentificationAmi Osh100% (2)
- Root Cause Analysis - ToolDocument11 paginiRoot Cause Analysis - ToolFouzan SoniwalaÎncă nu există evaluări
- Paper RCFA - Root Cause Failure AnalysisDocument7 paginiPaper RCFA - Root Cause Failure AnalysisMiguelÎncă nu există evaluări
- Elementary Quality Assurance ToolsDocument19 paginiElementary Quality Assurance ToolsignaunaqÎncă nu există evaluări
- Root Cause Analysis Day Course - HandoutsDocument67 paginiRoot Cause Analysis Day Course - Handoutsjps14Încă nu există evaluări
- Root Cause Analysis: Coronet Foods Pvt. LTDDocument103 paginiRoot Cause Analysis: Coronet Foods Pvt. LTDSaif Sultan0% (1)
- DNV Process Vs Occupational SafetyDocument17 paginiDNV Process Vs Occupational Safetymarsulex100% (1)
- RCA Methodology For Investigation 1686321388Document37 paginiRCA Methodology For Investigation 1686321388sravanivenkataÎncă nu există evaluări
- 2020 Failure Mode and Effects AnalysisDocument40 pagini2020 Failure Mode and Effects AnalysisEvri LiaÎncă nu există evaluări
- PSID Lessons Learned ASepedaDocument12 paginiPSID Lessons Learned ASepedaDiegoÎncă nu există evaluări
- LessonDocument2 paginiLessonCrislet ZatarainÎncă nu există evaluări
- Paired T-Test: AKA Dependent Sample T-Test and Repeated Measures T-TestDocument17 paginiPaired T-Test: AKA Dependent Sample T-Test and Repeated Measures T-TestSoh Mei LingÎncă nu există evaluări
- ColostomyDocument11 paginiColostomyRiddhi Mehta0% (1)
- Ec Childrenraceracism EnglishDocument21 paginiEc Childrenraceracism EnglishSyamsidar MajitÎncă nu există evaluări
- Activity ProposalDocument3 paginiActivity ProposalIvory Zaballa MancheteÎncă nu există evaluări
- Professional Education ReviewerDocument382 paginiProfessional Education ReviewerHanna Grace Honrade95% (37)
- CAO712S Schiffman CB10e IM 07 PDFDocument26 paginiCAO712S Schiffman CB10e IM 07 PDFSoyerji BeheraÎncă nu există evaluări
- Residential Security Coordinator QualificationsDocument1 paginăResidential Security Coordinator QualificationsAnonymous 97dbabE5Încă nu există evaluări
- Music and The BrainDocument6 paginiMusic and The BrainMalak KinaanÎncă nu există evaluări
- Instructor's Manual: This Package Contains: Levels 7 & 8Document117 paginiInstructor's Manual: This Package Contains: Levels 7 & 8Marcos Moreno Oliveira100% (1)
- Pengembangan Desain Pembelajaran Topik Peluang Berbasis Realistic Mathematics EducationDocument11 paginiPengembangan Desain Pembelajaran Topik Peluang Berbasis Realistic Mathematics EducationmegaÎncă nu există evaluări
- “Not Quite American: The Philippine Community in the United States (1907-1941)” in (Re)Presenting Filipino Americans, Asian American Studies Institute (A.A.S.I.)-University of Connecticut (U.S.A.), September 2002.Document9 pagini“Not Quite American: The Philippine Community in the United States (1907-1941)” in (Re)Presenting Filipino Americans, Asian American Studies Institute (A.A.S.I.)-University of Connecticut (U.S.A.), September 2002.Manuel L. Quezon III100% (1)
- CV in Format European - en FinalDocument2 paginiCV in Format European - en FinalVictor VSÎncă nu există evaluări
- Sdoc 02 28 SiDocument1 paginăSdoc 02 28 Sikevin.samsonÎncă nu există evaluări
- MOC Syllabus Harvard 2017Document8 paginiMOC Syllabus Harvard 2017Daniel Santos OrtegaÎncă nu există evaluări
- Parallel StructuresDocument28 paginiParallel StructuresSteven ReederÎncă nu există evaluări
- Position Paper Rubric Final Copy 2Document1 paginăPosition Paper Rubric Final Copy 2michaelscreenerÎncă nu există evaluări
- Detailed Lesson Plan in EnglishDocument10 paginiDetailed Lesson Plan in EnglishJeniva Ramos MalicdemÎncă nu există evaluări
- ASDFGHJKLDocument1 paginăASDFGHJKLRica Mae ChengSisterÎncă nu există evaluări
- 2010 Handbook Survey ResearchDocument51 pagini2010 Handbook Survey Researchec16043Încă nu există evaluări
- Detailed Lesson Plan in MAPEH 7Document7 paginiDetailed Lesson Plan in MAPEH 7Kesia100% (6)
- Research Center Recognition PDFDocument102 paginiResearch Center Recognition PDFaashay phirkeÎncă nu există evaluări
- P Science 4 Teacher's ResourceDocument154 paginiP Science 4 Teacher's ResourceShawky Mostafa100% (1)
- Makkar Ielts Writing Task 2Document4 paginiMakkar Ielts Writing Task 2Harpreet kaurÎncă nu există evaluări
- Constructing Objective Test Items:Simple Form: EDP 3501 Testing and Assessment in EducationDocument46 paginiConstructing Objective Test Items:Simple Form: EDP 3501 Testing and Assessment in EducationCik FarahÎncă nu există evaluări
- Module 4-Lesson 4.2Document9 paginiModule 4-Lesson 4.2Kel LumawanÎncă nu există evaluări
- Education in The United StatesDocument25 paginiEducation in The United StatesRichVosRolexÎncă nu există evaluări