S-ar putea să vă placă și
- Gram Positive BacilliDocument9 paginiGram Positive BacilliRovy JervisÎncă nu există evaluări
- Microbiology: Section IiDocument40 paginiMicrobiology: Section Iiparthibanb88100% (78)
- Microbial Culture MediaDocument9 paginiMicrobial Culture Mediaማላያላም ማላያላም100% (2)
- INFECTIONS IN DIALYSIS PATIENTS Basis & Prevention by Dr.T.V.Rao MDDocument48 paginiINFECTIONS IN DIALYSIS PATIENTS Basis & Prevention by Dr.T.V.Rao MDtummalapalli venkateswara raoÎncă nu există evaluări
- Artificial Intelligence in Healthcare Legal and Ethical Considerations Dr.T.V.Rao MDDocument34 paginiArtificial Intelligence in Healthcare Legal and Ethical Considerations Dr.T.V.Rao MDtummalapalli venkateswara raoÎncă nu există evaluări
- HOSPITAL ASSOCIATED Infections Overcoming Emerging Challenge by Dr.T.V.Rao MDDocument61 paginiHOSPITAL ASSOCIATED Infections Overcoming Emerging Challenge by Dr.T.V.Rao MDtummalapalli venkateswara raoÎncă nu există evaluări
- Mycology NotesDocument9 paginiMycology NotesIya Corpus100% (1)
- Influenza Teaching Current Update 2023 by Dr.T.V.Rao MDDocument100 paginiInfluenza Teaching Current Update 2023 by Dr.T.V.Rao MDtummalapalli venkateswara rao100% (1)
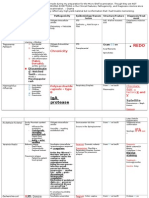
- High Yield - Bacteriology ChartsDocument9 paginiHigh Yield - Bacteriology ChartsAmirsalar EslamiÎncă nu există evaluări
- Medical Parasitology - FullDocument30 paginiMedical Parasitology - FullJesse Osborn100% (2)
- MicrobiologyDocument9 paginiMicrobiologyWenxinn JCFÎncă nu există evaluări
- Acid Fast Staining For TBDocument52 paginiAcid Fast Staining For TBtummalapalli venkateswara rao100% (2)
- Bacteriology HandoutsDocument30 paginiBacteriology HandoutsMarco Tolentino100% (8)
- Clinical Microbiology BacteriologyDocument25 paginiClinical Microbiology BacteriologyMunish DograÎncă nu există evaluări
- Clinical Microbiology 2Document20 paginiClinical Microbiology 2phuong mai leÎncă nu există evaluări
- Mycobacterium LectureDocument39 paginiMycobacterium LectureDegee GonzalesÎncă nu există evaluări
- Role of Personal Finance Towards Managing of Money - DraftaDocument35 paginiRole of Personal Finance Towards Managing of Money - DraftaAndrea Denise Lion100% (1)
- Summary of Diagnostic BacteriologyDocument45 paginiSummary of Diagnostic Bacteriologyomaromran100% (3)
- Skills Redux (10929123)Document23 paginiSkills Redux (10929123)AndrewCollas100% (1)
- LP Bacteria ChartDocument21 paginiLP Bacteria ChartTaman HoangÎncă nu există evaluări
- Mycology Lab3Document2 paginiMycology Lab3api-370057950% (2)
- Surgical Operation Theater StandardsDocument31 paginiSurgical Operation Theater Standardstummalapalli venkateswara raoÎncă nu există evaluări
- Roleplayer: The Accused Enchanted ItemsDocument68 paginiRoleplayer: The Accused Enchanted ItemsBarbie Turic100% (1)
- Sterilization and DisinfectionDocument10 paginiSterilization and DisinfectiondrugdrugÎncă nu există evaluări
- (123doc) - Toefl-Reading-Comprehension-Test-41Document8 pagini(123doc) - Toefl-Reading-Comprehension-Test-41Steve XÎncă nu există evaluări
- Infection Control in Burns PatietnsDocument41 paginiInfection Control in Burns Patietnstummalapalli venkateswara raoÎncă nu există evaluări
- BacteriologyDocument75 paginiBacteriologyHoward BarlomentoÎncă nu există evaluări
- Atlas Medical BacteriologyDocument104 paginiAtlas Medical BacteriologyradulusÎncă nu există evaluări
- IMS Objectives Targets 2Document2 paginiIMS Objectives Targets 2FaridUddin Ahmed100% (3)
- Microbiology BacteriaDocument4 paginiMicrobiology BacteriaFarahh ArshadÎncă nu există evaluări
- Bacteriology LectureDocument38 paginiBacteriology LectureAisle Malibiran Paler100% (1)
- Anaerobic Bacteria: Dept. of Microbiology Medical Faculty, Padjadjaran UniversityDocument52 paginiAnaerobic Bacteria: Dept. of Microbiology Medical Faculty, Padjadjaran UniversitySabrina Indri WardaniÎncă nu există evaluări
- Anaerobic Culture MethodsDocument75 paginiAnaerobic Culture Methodstummalapalli venkateswara rao0% (1)
- EnterobacteriaceaeDocument3 paginiEnterobacteriaceaeErnie G. Bautista II, RN, MDÎncă nu există evaluări
- Bacterial GeneticsDocument3 paginiBacterial GeneticsBobet Reña100% (2)
- Gram Negative RodsDocument8 paginiGram Negative RodsRuel Maddawin100% (1)
- Culture Media & Culture MethodsDocument60 paginiCulture Media & Culture MethodsGretchen Quimno Ayuson100% (2)
- MicrobiologyDocument40 paginiMicrobiologyRasty Baku100% (1)
- Medical MicrobiologyDocument41 paginiMedical Microbiologyapi-1991639950% (2)
- Clinical MicrobiologyDocument91 paginiClinical MicrobiologyDr. Jayesh Patidar67% (3)
- Diagnostic Bacteriology-Lab ReviewDocument45 paginiDiagnostic Bacteriology-Lab ReviewAtiya HajjajÎncă nu există evaluări
- INFECTION CONTROL TRENDS OF CHANGE by Dr.T.V.Rao MDDocument25 paginiINFECTION CONTROL TRENDS OF CHANGE by Dr.T.V.Rao MDtummalapalli venkateswara rao100% (1)
- BacteriologyDocument13 paginiBacteriologyGlydenne Glaire Poncardas Gayam33% (3)
- Screening For MRSA by Dr.T.V.Rao MDDocument30 paginiScreening For MRSA by Dr.T.V.Rao MDtummalapalli venkateswara raoÎncă nu există evaluări
- Viral Pathogenesis: From Basics to Systems BiologyDe la EverandViral Pathogenesis: From Basics to Systems BiologyEvaluare: 5 din 5 stele5/5 (2)
- Taxonomic Guide to Infectious Diseases: Understanding the Biologic Classes of Pathogenic OrganismsDe la EverandTaxonomic Guide to Infectious Diseases: Understanding the Biologic Classes of Pathogenic OrganismsEvaluare: 5 din 5 stele5/5 (1)
- Anaerobic Bacteriology: Clinical and Laboratory PracticeDe la EverandAnaerobic Bacteriology: Clinical and Laboratory PracticeÎncă nu există evaluări
- Laboratory Detection of ESBLDocument69 paginiLaboratory Detection of ESBLtummalapalli venkateswara rao100% (1)
- Microbiology PDFDocument40 paginiMicrobiology PDFputri tyas100% (1)
- Chapter 1 Microbiology PDFDocument79 paginiChapter 1 Microbiology PDFpizza100% (1)
- Textbook of Medical Parasitology Protozoology HelmDocument2 paginiTextbook of Medical Parasitology Protozoology HelmAnge OuedraogoÎncă nu există evaluări
- Micrology and Parasitology ReviewerDocument44 paginiMicrology and Parasitology Reviewermarjourie cadampog100% (1)
- Anaerobic BacteriaDocument2 paginiAnaerobic BacteriaAbhugz MarceloÎncă nu există evaluări
- Clinical ChemistryDocument1 paginăClinical Chemistryaiai0% (1)
- 4th Shifting Micro Lab ReviewerDocument154 pagini4th Shifting Micro Lab ReviewerJade MonrealÎncă nu există evaluări
- MLT Student NotesDocument5 paginiMLT Student NotesClaire GonzalesÎncă nu există evaluări
- Introduction To MycologyDocument26 paginiIntroduction To MycologyOsannah Irish InsongÎncă nu există evaluări
- General Microbiology (Chapter 3)Document18 paginiGeneral Microbiology (Chapter 3)Ashraf OsmanÎncă nu există evaluări
- Anaerobic BacteriaDocument27 paginiAnaerobic Bacteriaapi-26826496100% (3)
- Leukaemoid Reaction Lecture by DRDocument35 paginiLeukaemoid Reaction Lecture by DRapi-273068056100% (1)
- Microbial Products of Potential Importance - Product / Activity Examples ProductsDocument10 paginiMicrobial Products of Potential Importance - Product / Activity Examples ProductsShveta Jaishankar Iyer100% (4)
- 1.04 Biochemistry Trans - EnzymesDocument11 pagini1.04 Biochemistry Trans - EnzymesApril AramÎncă nu există evaluări
- MALDI-ToF in Clinical MicrobiologyDocument39 paginiMALDI-ToF in Clinical Microbiologytummalapalli venkateswara rao100% (1)
- Microbiology Notes Chapers 1-2Document3 paginiMicrobiology Notes Chapers 1-2dinkinpdÎncă nu există evaluări
- Virology ReviewDocument21 paginiVirology ReviewfrabziÎncă nu există evaluări
- Viral ReplicationDocument1 paginăViral ReplicationMoh'd Ghanayem100% (1)
- Types of FermentersDocument3 paginiTypes of FermentersHoney krishnaÎncă nu există evaluări
- Microbio Lec 1 - Bacterial Morphology and Ultra StructureDocument8 paginiMicrobio Lec 1 - Bacterial Morphology and Ultra Structureapi-3743217100% (3)
- Microbiology PDFDocument71 paginiMicrobiology PDFDanny Alexander TullumeÎncă nu există evaluări
- Safe Blood: Purifying the Nations Blood Supply in the Age of ADe la EverandSafe Blood: Purifying the Nations Blood Supply in the Age of AÎncă nu există evaluări
- GRAM STAINING AND CLINICAL UTILITY by Dr.T.V.Rao MDDocument2 paginiGRAM STAINING AND CLINICAL UTILITY by Dr.T.V.Rao MDtummalapalli venkateswara raoÎncă nu există evaluări
- Need For Clinical Microbiologists by Dr.T.V.Rao MDDocument2 paginiNeed For Clinical Microbiologists by Dr.T.V.Rao MDtummalapalli venkateswara rao100% (1)
- MDR - TB Emerging Methods in Diagnosis Dr.T.V.Rao MDDocument2 paginiMDR - TB Emerging Methods in Diagnosis Dr.T.V.Rao MDtummalapalli venkateswara raoÎncă nu există evaluări
- Who Is Killing Modern Medicine in IndiaDocument3 paginiWho Is Killing Modern Medicine in Indiatummalapalli venkateswara raoÎncă nu există evaluări
- MALDI-ToF in Clinical MicrobiologyDocument39 paginiMALDI-ToF in Clinical Microbiologytummalapalli venkateswara rao100% (1)
- MDR - TB FACTS AND CONCERNS BY Dr.T.V.Rao MDDocument33 paginiMDR - TB FACTS AND CONCERNS BY Dr.T.V.Rao MDtummalapalli venkateswara raoÎncă nu există evaluări
- Elizabethkingia Meningoseptica An Emerging Infection by Dr.T.V.Rao MDDocument28 paginiElizabethkingia Meningoseptica An Emerging Infection by Dr.T.V.Rao MDtummalapalli venkateswara raoÎncă nu există evaluări
- Health Care Associated Infections Creating Drug Resistance AtlasDocument46 paginiHealth Care Associated Infections Creating Drug Resistance Atlastummalapalli venkateswara raoÎncă nu există evaluări
- Auditing Hospital Associated InfectionsDocument59 paginiAuditing Hospital Associated Infectionstummalapalli venkateswara raoÎncă nu există evaluări
- AUDITING ANTIBIOGRAMS by Dr.T.V.RaoMDDocument55 paginiAUDITING ANTIBIOGRAMS by Dr.T.V.RaoMDtummalapalli venkateswara rao100% (1)
- MDR-TB An Update by Dr.T.V.Rao MDDocument43 paginiMDR-TB An Update by Dr.T.V.Rao MDtummalapalli venkateswara raoÎncă nu există evaluări
- ZIKA VIRUS INFECTION Emerging Public Health ConcernDocument36 paginiZIKA VIRUS INFECTION Emerging Public Health Concerntummalapalli venkateswara rao100% (1)
- Revisiting Blood CulturingDocument2 paginiRevisiting Blood Culturingtummalapalli venkateswara raoÎncă nu există evaluări
- Surgical Gloves in Health CareDocument29 paginiSurgical Gloves in Health Caretummalapalli venkateswara raoÎncă nu există evaluări
- Medical Microbiology in Crisis in IndiaDocument4 paginiMedical Microbiology in Crisis in Indiatummalapalli venkateswara raoÎncă nu există evaluări
- Read While Being Blind.. Braille's Alphabet: Be Aware and Active !Document3 paginiRead While Being Blind.. Braille's Alphabet: Be Aware and Active !bitermanÎncă nu există evaluări
- Introduction-: Microprocessor 68000Document13 paginiIntroduction-: Microprocessor 68000margyaÎncă nu există evaluări
- Law of EvidenceDocument14 paginiLaw of EvidenceIsha ChavanÎncă nu există evaluări
- Chemistry: Crash Course For JEE Main 2020Document18 paginiChemistry: Crash Course For JEE Main 2020Sanjeeb KumarÎncă nu există evaluări
- SMC 2D CADLibrary English 1Document590 paginiSMC 2D CADLibrary English 1Design IPGEÎncă nu există evaluări
- Retailing in IndiaDocument11 paginiRetailing in IndiaVinod MalkarÎncă nu există evaluări
- Movie Piracy in Ethiopian CinemaDocument22 paginiMovie Piracy in Ethiopian CinemaBehailu Shiferaw MihireteÎncă nu există evaluări
- Stearns 87700 Series Parts ListDocument4 paginiStearns 87700 Series Parts ListYorkistÎncă nu există evaluări
- 3 Carbohydrates' StructureDocument33 pagini3 Carbohydrates' StructureDilan TeodoroÎncă nu există evaluări
- User S Manual AURORA 1.2K - 2.2KDocument288 paginiUser S Manual AURORA 1.2K - 2.2KEprom ServisÎncă nu există evaluări
- DPSD ProjectDocument30 paginiDPSD ProjectSri NidhiÎncă nu există evaluări
- Hole CapacityDocument2 paginiHole CapacityAbdul Hameed OmarÎncă nu există evaluări
- Organizational ConflictDocument22 paginiOrganizational ConflictTannya AlexandraÎncă nu există evaluări
- ME Eng 8 Q1 0101 - SG - African History and LiteratureDocument13 paginiME Eng 8 Q1 0101 - SG - African History and Literaturerosary bersanoÎncă nu există evaluări
- WEB DESIGN WITH AUSTINE-converted-1Document9 paginiWEB DESIGN WITH AUSTINE-converted-1JayjayÎncă nu există evaluări
- LTE Networks Engineering Track Syllabus Overview - 23 - 24Document4 paginiLTE Networks Engineering Track Syllabus Overview - 23 - 24Mohamed SamiÎncă nu există evaluări
- SMR 13 Math 201 SyllabusDocument2 paginiSMR 13 Math 201 SyllabusFurkan ErisÎncă nu există evaluări
- Environmental Economics Pollution Control: Mrinal Kanti DuttaDocument253 paginiEnvironmental Economics Pollution Control: Mrinal Kanti DuttashubhamÎncă nu există evaluări
- Chemistry Form 4 Daily Lesson Plan - CompressDocument3 paginiChemistry Form 4 Daily Lesson Plan - Compressadila ramlonÎncă nu există evaluări
- Career Essay 1Document2 paginiCareer Essay 1api-572592063Încă nu există evaluări
- Functions in C++Document23 paginiFunctions in C++Abhishek ModiÎncă nu există evaluări
- Spesifikasi PM710Document73 paginiSpesifikasi PM710Phan'iphan'Încă nu există evaluări
- Carob-Tree As CO2 Sink in The Carbon MarketDocument5 paginiCarob-Tree As CO2 Sink in The Carbon MarketFayssal KartobiÎncă nu există evaluări
- PR KehumasanDocument14 paginiPR KehumasanImamÎncă nu există evaluări
- An Exploration of The Ethno-Medicinal Practices Among Traditional Healers in Southwest Cebu, PhilippinesDocument7 paginiAn Exploration of The Ethno-Medicinal Practices Among Traditional Healers in Southwest Cebu, PhilippinesleecubongÎncă nu există evaluări