S-ar putea să vă placă și
- Dr. Jaddou - Research DesignsDocument36 paginiDr. Jaddou - Research DesignsNur Hamizah Md FuziÎncă nu există evaluări
- Presentation Abdominal Pain, MassesDocument36 paginiPresentation Abdominal Pain, MassesNur Hamizah Md FuziÎncă nu există evaluări
- Prof. Khafaji - Oswego.Document24 paginiProf. Khafaji - Oswego.Nur Hamizah Md Fuzi86% (7)
- Prof. Khafaji - Oswego.Document24 paginiProf. Khafaji - Oswego.Nur Hamizah Md Fuzi86% (7)
- Cardiovascular System SX HXDocument38 paginiCardiovascular System SX HXNur Hamizah Md FuziÎncă nu există evaluări
- Maternal Mortality in JordanDocument67 paginiMaternal Mortality in JordanNur Hamizah Md FuziÎncă nu există evaluări
- GI History IntroductoryDocument74 paginiGI History IntroductoryNur Hamizah Md FuziÎncă nu există evaluări
- Abdominal ExaminationDocument70 paginiAbdominal ExaminationNur Hamizah Md FuziÎncă nu există evaluări
- Respiratory ExaminationDocument59 paginiRespiratory ExaminationNur Hamizah Md FuziÎncă nu există evaluări
- CVS MCQDocument14 paginiCVS MCQNur Hamizah Md FuziÎncă nu există evaluări
- Clinical History: Professor Niazy Abu Farsakh Jordan University of Science and TechnologyDocument31 paginiClinical History: Professor Niazy Abu Farsakh Jordan University of Science and TechnologyNur Hamizah Md FuziÎncă nu există evaluări
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (119)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Infections in Pregnant WomenDocument3 paginiInfections in Pregnant Womentummalapalli venkateswara raoÎncă nu există evaluări
- TAREA 2 Marlin Rivas LDocument9 paginiTAREA 2 Marlin Rivas Lmarlin lobonÎncă nu există evaluări
- QuadriplegiaDocument20 paginiQuadriplegiashahsushmita02Încă nu există evaluări
- Early Diagnosis of NeoplasisDocument25 paginiEarly Diagnosis of NeoplasisDanielaÎncă nu există evaluări
- TorchesDocument23 paginiTorchesErrold Joseph LahaganÎncă nu există evaluări
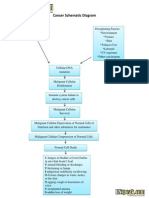
- Cancer Schematic DiagramDocument1 paginăCancer Schematic DiagramCyrus De Asis100% (4)
- Louisiana Couple Sues Pelahatchie Water Park After Daughter Allegedly Contracts E. ColiDocument9 paginiLouisiana Couple Sues Pelahatchie Water Park After Daughter Allegedly Contracts E. ColiWLBT NewsÎncă nu există evaluări
- 5-Neuro MCQs Final UnsolvedDocument29 pagini5-Neuro MCQs Final UnsolvedOsman Somi0% (2)
- Antibiotic Susceptibility Patterns of Methicillin Resistant Staphyl - PDF NIHDocument5 paginiAntibiotic Susceptibility Patterns of Methicillin Resistant Staphyl - PDF NIHzia ul RahmanÎncă nu există evaluări
- CHN CompreDocument11 paginiCHN CompreAnn Aquino IIÎncă nu există evaluări
- DR - REVATI - IMMUNE MEDIATED DISEASES OF OROFACIAL REGION - RevatiDocument72 paginiDR - REVATI - IMMUNE MEDIATED DISEASES OF OROFACIAL REGION - RevatiNanik AndianiÎncă nu există evaluări
- Jurnal SinusitisDocument49 paginiJurnal SinusitisAramanda Dian100% (1)
- Sars-Cov-2 Variant of Concern Omicron: Update OnDocument24 paginiSars-Cov-2 Variant of Concern Omicron: Update OnDanna AflahÎncă nu există evaluări
- COURSE TITLE - NCM 113Document40 paginiCOURSE TITLE - NCM 113Geevee Naganag VentulaÎncă nu există evaluări
- Surviving Sepsis Campaign Hour 1 BundleDocument5 paginiSurviving Sepsis Campaign Hour 1 BundleNadine Noelle AgraviadorÎncă nu există evaluări
- Prep 2018Document970 paginiPrep 2018Dr. Faten AlKatebÎncă nu există evaluări
- Nursing Care Plan - Acute Pain Related To Surgical IncisionDocument2 paginiNursing Care Plan - Acute Pain Related To Surgical IncisionCamilogs80% (10)
- Presentation On WalnutDocument5 paginiPresentation On WalnutSheikh JeelaniÎncă nu există evaluări
- Risk For Infection Related To Inadequate Primary Defenses: Broken SkinDocument2 paginiRisk For Infection Related To Inadequate Primary Defenses: Broken SkinReylan Garcia100% (8)
- Management of Acute Glomerulonephritis in Children: Children's Services Medical GuidelinesDocument7 paginiManagement of Acute Glomerulonephritis in Children: Children's Services Medical GuidelinesdaypranitaÎncă nu există evaluări
- Block K GMC W ExplanationDocument15 paginiBlock K GMC W ExplanationSaad KhanÎncă nu există evaluări
- Chelidonim VS NuxvomDocument3 paginiChelidonim VS Nuxvomtakne_007Încă nu există evaluări
- Pre AssessmentDocument26 paginiPre AssessmentAbe Estrada EnanoÎncă nu există evaluări
- Case Study Htm400Document6 paginiCase Study Htm400maizatul rosniÎncă nu există evaluări
- Correlation of Mammographic and Histopathological Characteristics of Breast LesionsDocument8 paginiCorrelation of Mammographic and Histopathological Characteristics of Breast LesionsIJAR JOURNALÎncă nu există evaluări
- 2020 Putri - STUDI LITERATUR EFEKTIVITAS PENGGUNAAN MASKER KAINDocument9 pagini2020 Putri - STUDI LITERATUR EFEKTIVITAS PENGGUNAAN MASKER KAINHandy NugrohoÎncă nu există evaluări
- Community Health Nursing ProcessDocument15 paginiCommunity Health Nursing ProcessLheane Marley LopenaÎncă nu există evaluări
- Test Questionnaire For Needs AnalysisDocument5 paginiTest Questionnaire For Needs AnalysisYenyen Quirog-PalmesÎncă nu există evaluări
- Dr. Wisman's Hematology ReferenceDocument38 paginiDr. Wisman's Hematology ReferenceYpoxazÎncă nu există evaluări
- WA DSHS Report On Enumclaw Health and Rehab's COVID-19 ProceduresDocument11 paginiWA DSHS Report On Enumclaw Health and Rehab's COVID-19 ProceduresRay StillÎncă nu există evaluări