S-ar putea să vă placă și
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Current Methods of Shade Matching in Dentistry A Review of The Supporting Literature PDFDocument6 paginiCurrent Methods of Shade Matching in Dentistry A Review of The Supporting Literature PDFSueChen TanÎncă nu există evaluări
- Questions in OphthalmologyDocument27 paginiQuestions in Ophthalmologyeyepage100% (6)
- The Psychology of Color in Film (Intro To Drama)Document43 paginiThe Psychology of Color in Film (Intro To Drama)jotadeÎncă nu există evaluări
- How Is IgA Nephropathy TreatedDocument2 paginiHow Is IgA Nephropathy TreatedRees SkaranÎncă nu există evaluări
- How Is IgA Nephropathy TreatedDocument2 paginiHow Is IgA Nephropathy TreatedRees SkaranÎncă nu există evaluări
- How To Make A Rainbow CakeDocument2 paginiHow To Make A Rainbow CakeRees SkaranÎncă nu există evaluări
- Chapter 5 Measures of VariabilityDocument23 paginiChapter 5 Measures of VariabilityRees SkaranÎncă nu există evaluări
- Chapter 19 Chi-SquareDocument22 paginiChapter 19 Chi-SquareRees SkaranÎncă nu există evaluări
- Chapter 2 Basic ConceptsDocument14 paginiChapter 2 Basic ConceptsRees SkaranÎncă nu există evaluări
- Chapter 1 IntroductionDocument8 paginiChapter 1 IntroductionRees Skaran0% (1)
- Basic Counseling Skills-WebDocument9 paginiBasic Counseling Skills-Webjelb25Încă nu există evaluări
- Data Ujian Osce Biostatistik Blok 20Document8 paginiData Ujian Osce Biostatistik Blok 20Trizky Nataza PutraÎncă nu există evaluări
- How To Make A Rainbow CakeDocument2 paginiHow To Make A Rainbow CakeRees SkaranÎncă nu există evaluări
- How To Make A Rainbow CakeDocument2 paginiHow To Make A Rainbow CakeRees SkaranÎncă nu există evaluări
- Case Report MineDocument21 paginiCase Report MineRees SkaranÎncă nu există evaluări
- Hemiplegi Sinistra FlaksidDocument19 paginiHemiplegi Sinistra FlaksidRees SkaranÎncă nu există evaluări
- Pensi Bulan: Click To Edit Master Subtitle StyleDocument17 paginiPensi Bulan: Click To Edit Master Subtitle StyleRees SkaranÎncă nu există evaluări
- Vasan Eye CareDocument13 paginiVasan Eye CareGokul BalajiÎncă nu există evaluări
- 12-2 - Fri - vision-hearing-EQDocument13 pagini12-2 - Fri - vision-hearing-EQTyler DeanÎncă nu există evaluări
- Arts-Mapeh (3RD Quarter)Document50 paginiArts-Mapeh (3RD Quarter)Sheilla Semacio PlazoÎncă nu există evaluări
- Architectural Photography Presentation - Brett Ryan StudiosDocument113 paginiArchitectural Photography Presentation - Brett Ryan StudiosBrett Ryan Studios100% (2)
- Colors and ColorcodesDocument5 paginiColors and Colorcodesandrea carolina serrrato chinchillaÎncă nu există evaluări
- H R Textile Mills Limited: Finished Batch Deliver From 1/1/2014 To 1/8/2014Document12 paginiH R Textile Mills Limited: Finished Batch Deliver From 1/1/2014 To 1/8/2014Al Arafat RummanÎncă nu există evaluări
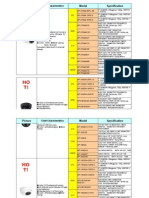
- 499 Spec of DS-2CE16C2T-VFIR3 PDFDocument2 pagini499 Spec of DS-2CE16C2T-VFIR3 PDFPaul AlexandruÎncă nu există evaluări
- Eye Diagnostic Points - McqsDocument21 paginiEye Diagnostic Points - McqsMuhammad AwaisÎncă nu există evaluări
- Digital SLR Photography 2013-11Document164 paginiDigital SLR Photography 2013-11WillimSmith100% (2)
- Goat SimulatorDocument26 paginiGoat SimulatorNorman MikhailÎncă nu există evaluări
- PHOTOGRAPHY PPDocument27 paginiPHOTOGRAPHY PPPau TorrefielÎncă nu există evaluări
- Iris Recognition Using MATLABDocument9 paginiIris Recognition Using MATLABmanojmuthyalaÎncă nu există evaluări
- CCTVDocument4 paginiCCTVSquarescreensÎncă nu există evaluări
- Foreign Body in Eye - Dr. Murali Mohan GurramDocument10 paginiForeign Body in Eye - Dr. Murali Mohan GurramDr. Murali Mohan Gurram MS,DNB,FRCS,MCh,FICO,FRVS,FAGE,MNAMS,FIMSA,CCN,PGDCA100% (1)
- Efficacy and Safety of A Soft Contact Lens To Control MyopiaprogressionDocument8 paginiEfficacy and Safety of A Soft Contact Lens To Control MyopiaprogressionAmandaÎncă nu există evaluări
- En CLB41 Nasse LensNames DistagonDocument15 paginiEn CLB41 Nasse LensNames DistagonseifadiazÎncă nu există evaluări
- PhotographyDocument202 paginiPhotographyErichvonGotha92% (12)
- Titmus Vision Screener V4Document1 paginăTitmus Vision Screener V4rodrigo rodriguez pachonÎncă nu există evaluări
- Tone MappingDocument7 paginiTone MappingMahvish FatimaÎncă nu există evaluări
- Empowerment Technology 10 FinalDocument9 paginiEmpowerment Technology 10 Finalandy gamingÎncă nu există evaluări
- ACP - Alcopanel 2Document4 paginiACP - Alcopanel 2Bilher SihombingÎncă nu există evaluări
- p4 Create Original Graphics Images To Meet A Defined User NeedDocument4 paginip4 Create Original Graphics Images To Meet A Defined User Needapi-300823967Încă nu există evaluări
- Image Segmentation Digital Image ProcessingDocument44 paginiImage Segmentation Digital Image Processingnaveednad2003556100% (1)
- Clinical Optics: Basic and Clinical Science CourseDocument18 paginiClinical Optics: Basic and Clinical Science CourseYasminSolbergÎncă nu există evaluări
- Basic Optics - Dispensing & OptometricDocument4 paginiBasic Optics - Dispensing & OptometricAryan PatelÎncă nu există evaluări
- Artificial EyeDocument31 paginiArtificial Eyeapi-19937584Încă nu există evaluări