S-ar putea să vă placă și
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- ARMD StudyDocument40 paginiARMD StudyAnumeha JindalÎncă nu există evaluări
- Future Implications of Anti VegfDocument6 paginiFuture Implications of Anti VegfAnumeha JindalÎncă nu există evaluări
- Micronutrients and AgeDocument9 paginiMicronutrients and AgeAnumeha JindalÎncă nu există evaluări
- Inflammation in Dry Age Related Macular DegenrationDocument11 paginiInflammation in Dry Age Related Macular DegenrationAnumeha JindalÎncă nu există evaluări
- Amsler Grid 1Document9 paginiAmsler Grid 1Anumeha JindalÎncă nu există evaluări
- Amsler's GridDocument1 paginăAmsler's GridAnumeha JindalÎncă nu există evaluări
- Anti VegfDocument3 paginiAnti VegfAnumeha Jindal100% (1)
- Exquisite Sandalwood Massage OilDocument1 paginăExquisite Sandalwood Massage OilAnumeha JindalÎncă nu există evaluări
- Herbal Recipes For AromatherapyDocument3 paginiHerbal Recipes For AromatherapyAnumeha Jindal100% (4)
- Age Related Macular DegenerationDocument21 paginiAge Related Macular DegenerationAnumeha JindalÎncă nu există evaluări
- Creating Your Own Blogger Template From Scratch, Sort ofDocument11 paginiCreating Your Own Blogger Template From Scratch, Sort ofAnumeha JindalÎncă nu există evaluări
- Poster Design in CorelDrawDocument72 paginiPoster Design in CorelDrawAnumeha Jindal50% (2)
- ARMD GeneticsDocument9 paginiARMD GeneticsAnumeha JindalÎncă nu există evaluări
- Flower Blossom Massage Oil RecipeDocument1 paginăFlower Blossom Massage Oil RecipeAnumeha JindalÎncă nu există evaluări
- Essential Oil SubstitutesDocument13 paginiEssential Oil SubstitutesAnumeha JindalÎncă nu există evaluări
- From The Aromatherapy Recipe Files Volume 24Document3 paginiFrom The Aromatherapy Recipe Files Volume 24Anumeha JindalÎncă nu există evaluări
- Exotic Massage Oil RecipeDocument1 paginăExotic Massage Oil RecipeAnumeha JindalÎncă nu există evaluări
- From The Aromatherapy Recipe Files Volume 20Document3 paginiFrom The Aromatherapy Recipe Files Volume 20Anumeha JindalÎncă nu există evaluări
- From The Aromatherapy Recipe Files Volume 22Document3 paginiFrom The Aromatherapy Recipe Files Volume 22Anumeha JindalÎncă nu există evaluări
- Insomnia Relief Massage Oil RecipeDocument1 paginăInsomnia Relief Massage Oil RecipeAnumeha JindalÎncă nu există evaluări
- From The Aromatherapy Recipe FilesDocument2 paginiFrom The Aromatherapy Recipe FilesAnumeha JindalÎncă nu există evaluări
- From The Aromatherapy Recipe Files Volume 21Document3 paginiFrom The Aromatherapy Recipe Files Volume 21Anumeha JindalÎncă nu există evaluări
- How To Apply Essential Oils For Chakra BalancingDocument2 paginiHow To Apply Essential Oils For Chakra BalancingAnumeha Jindal100% (1)
- The Chakras and Essential OilsDocument10 paginiThe Chakras and Essential OilsAnumeha Jindal100% (4)
- Some Substitutions For Essential OilsDocument1 paginăSome Substitutions For Essential OilsAnumeha JindalÎncă nu există evaluări
- Other Aromatherapy RecpiesDocument13 paginiOther Aromatherapy RecpiesAnumeha JindalÎncă nu există evaluări
- Meditating With Essential OilsDocument2 paginiMeditating With Essential OilsAnumeha JindalÎncă nu există evaluări
- Recipes Using JojobaDocument1 paginăRecipes Using JojobaAnumeha JindalÎncă nu există evaluări
- The Third Eye (Brow) Chakra and Essential OilsDocument2 paginiThe Third Eye (Brow) Chakra and Essential OilsAnumeha JindalÎncă nu există evaluări
- Essential Oil of The Month: SandlewoodDocument2 paginiEssential Oil of The Month: SandlewoodAnumeha Jindal0% (1)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- International Journal of Surgery Case ReportsDocument4 paginiInternational Journal of Surgery Case Reportshussein_faourÎncă nu există evaluări
- Fibrous Dysplasia of BoneDocument31 paginiFibrous Dysplasia of Bonet.babyÎncă nu există evaluări
- Ocd Presentation 3Document11 paginiOcd Presentation 3api-387888714Încă nu există evaluări
- Clinical Approach To The Dysmorphic Child-R-1Document108 paginiClinical Approach To The Dysmorphic Child-R-1Drbhupeshwari Gour100% (1)
- Pediatric Case StudyDocument29 paginiPediatric Case Studyapi-296281683Încă nu există evaluări
- Ect BrochureDocument2 paginiEct Brochureapi-283706202Încă nu există evaluări
- Hyper Parathyroid IsmDocument7 paginiHyper Parathyroid IsmEllene Mae Dejapa VillasisÎncă nu există evaluări
- Diabetes MellitusDocument41 paginiDiabetes MellitusYuttapol PimpisonÎncă nu există evaluări
- Coding TechniquesDocument16 paginiCoding TechniquesShane BridgesÎncă nu există evaluări
- Laboratory Tests To Evaluate Fluid StatusDocument52 paginiLaboratory Tests To Evaluate Fluid StatusLester Exconde Alfonso0% (1)
- SurgerySuturePatternsT SissenerDocument5 paginiSurgerySuturePatternsT SissenerPitche Tomale100% (1)
- Beddis2014 Management of Deep Overbite PDFDocument7 paginiBeddis2014 Management of Deep Overbite PDFnithya_sendhilÎncă nu există evaluări
- Bryan 3-24-17Document12 paginiBryan 3-24-17Bryan VandentoornÎncă nu există evaluări
- Clostridium Difficile Infection and Fecal BacteriotherapyDocument9 paginiClostridium Difficile Infection and Fecal BacteriotherapyAnonymous nEC4alrPjGÎncă nu există evaluări
- NaloxoneDocument3 paginiNaloxoneTracyÎncă nu există evaluări
- Cobas C 311 enDocument12 paginiCobas C 311 enCássio Menezes GodóiÎncă nu există evaluări
- 02 Full Crown PreparationDocument35 pagini02 Full Crown PreparationSurgaBetariJelita100% (1)
- Information SystemDocument15 paginiInformation Systemzanmatto22Încă nu există evaluări
- Cardiac Rehabilitation For Patients With Coronary Artery Disease: A Practical Guide To Enhance Patient Outcomes Through Continuity of CareDocument7 paginiCardiac Rehabilitation For Patients With Coronary Artery Disease: A Practical Guide To Enhance Patient Outcomes Through Continuity of CareAnnisa Tri NastitiÎncă nu există evaluări
- 6 Concept of Mental Health and Well BeingDocument24 pagini6 Concept of Mental Health and Well BeingJayward Babaran Bayug100% (2)
- Pediatric Basic Life SupportDocument50 paginiPediatric Basic Life SupportnurmauliarizkyÎncă nu există evaluări
- Chronic Renal FailureDocument18 paginiChronic Renal FailureJoan Carla BocoÎncă nu există evaluări
- My Experience With Topical Homoeopathic Application in A Case of Stage Iv Decubitus UlcerDocument5 paginiMy Experience With Topical Homoeopathic Application in A Case of Stage Iv Decubitus UlcerHomoeopathic PulseÎncă nu există evaluări
- Suggamadex Remifentanyl PalonosetronDocument28 paginiSuggamadex Remifentanyl PalonosetronSai TejeswiÎncă nu există evaluări
- Somalia Launches First Ever-Cleft Lip and Palate Surgery ClinicDocument4 paginiSomalia Launches First Ever-Cleft Lip and Palate Surgery ClinicAMISOM Public Information ServicesÎncă nu există evaluări
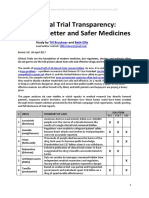
- Clinical Trial Transparency - A Key To Better and Safer Medicines (Till Bruckner and Beth Ellis 2017)Document21 paginiClinical Trial Transparency - A Key To Better and Safer Medicines (Till Bruckner and Beth Ellis 2017)Till BrucknerÎncă nu există evaluări
- Temporary Flexible Removable Partial DentureDocument4 paginiTemporary Flexible Removable Partial DentureenipurwantiÎncă nu există evaluări
- Respiratory BubblingDocument7 paginiRespiratory BubblingErwin SiregarÎncă nu există evaluări
- A Case StudyDocument30 paginiA Case StudyJie BandelariaÎncă nu există evaluări