S-ar putea să vă placă și
- Puerperium and Its Management 1Document35 paginiPuerperium and Its Management 1Elvis100% (2)
- New NORMAL PUERPERIUMDocument21 paginiNew NORMAL PUERPERIUMvarshaÎncă nu există evaluări
- Normal PuerperiumDocument23 paginiNormal Puerperiumnaga maniÎncă nu există evaluări
- Manual Removal of The PlacentaDocument2 paginiManual Removal of The PlacentavalpretlÎncă nu există evaluări
- Post Partum HemorhageDocument7 paginiPost Partum HemorhageLithiya JoseÎncă nu există evaluări
- Uterine Malformations PDFDocument6 paginiUterine Malformations PDFsaritha OrugantiÎncă nu există evaluări
- Polyhydramnios and OlygohydramniosDocument32 paginiPolyhydramnios and Olygohydramniosafifurrahman_rizalÎncă nu există evaluări
- Abruption PacentaDocument6 paginiAbruption PacentaKondapavuluru JyothiÎncă nu există evaluări
- Vesicular MoleDocument46 paginiVesicular Moledhisazainita0% (1)
- Normal DeliveryDocument41 paginiNormal DeliveryAliÎncă nu există evaluări
- HydramniosDocument31 paginiHydramniosSpandana DepuruÎncă nu există evaluări
- Abortion II ND Yr MSC NursingDocument121 paginiAbortion II ND Yr MSC Nursingesthereugenia100% (1)
- Management of LabourDocument16 paginiManagement of LabourAlbert MusinguziÎncă nu există evaluări
- Physiology of Normal LabourDocument29 paginiPhysiology of Normal LabournamitaÎncă nu există evaluări
- Genital Tract InjuriesDocument19 paginiGenital Tract InjuriesMarvella Nongkhar100% (1)
- Augmentation and IOLDocument22 paginiAugmentation and IOLvani reddyÎncă nu există evaluări
- Retained Placenta After Vaginal Birth and Length of The Third Stage of Labor - UpToDateDocument19 paginiRetained Placenta After Vaginal Birth and Length of The Third Stage of Labor - UpToDateHartanto Lie100% (1)
- Malpresentation and Malposition - ShoulderDocument5 paginiMalpresentation and Malposition - ShoulderNishaThakuri100% (1)
- Maternal, Morbidity, Mortality and Fertility RatesDocument18 paginiMaternal, Morbidity, Mortality and Fertility Ratesmadhu.BÎncă nu există evaluări
- Partograph DR OdofinDocument61 paginiPartograph DR OdofinEkiran BabajideÎncă nu există evaluări
- Perineal TearsDocument44 paginiPerineal TearsMagic_OverÎncă nu există evaluări
- Induction of LabourDocument18 paginiInduction of LabourNihal ZaidiÎncă nu există evaluări
- Antepartum HaemorrhageDocument18 paginiAntepartum HaemorrhageOjambo Flavia100% (1)
- Prolonged LabourDocument36 paginiProlonged LabourQuay Kar Ying100% (3)
- Malpresentation and Malposition - BreechDocument21 paginiMalpresentation and Malposition - BreechNishaThakuri100% (1)
- Minor Disorders of PregnancyDocument28 paginiMinor Disorders of PregnancyAbdullahi Suleiman Maka100% (1)
- Ectopic PregnancyDocument10 paginiEctopic PregnancyXo Yem0% (1)
- Physiological Changes During Second Stage of LabourDocument44 paginiPhysiological Changes During Second Stage of LabourTami SelviÎncă nu există evaluări
- 26a. Post Partum HemorrhageDocument35 pagini26a. Post Partum HemorrhageAubrey100% (1)
- PuerperiumDocument28 paginiPuerperiumZarlyn MirafloresÎncă nu există evaluări
- Postpartum ComplicationsDocument26 paginiPostpartum ComplicationsSharinah Ainee Sabalburo PasandalanÎncă nu există evaluări
- Abortion: TH THDocument36 paginiAbortion: TH THdimlyÎncă nu există evaluări
- AbortionsDocument99 paginiAbortionsAGERI PUSHPALATHAÎncă nu există evaluări
- CPDDocument14 paginiCPDmaezuÎncă nu există evaluări
- Puerperal SepsisDocument45 paginiPuerperal SepsisKalo kajiÎncă nu există evaluări
- Effects of Maternal Drugs On The FetusDocument9 paginiEffects of Maternal Drugs On The FetusJennifer DixonÎncă nu există evaluări
- PuerperiumDocument36 paginiPuerperiumGirish WaruÎncă nu există evaluări
- Genital Tract InjuriesDocument37 paginiGenital Tract InjuriesShady Abdelbari83% (6)
- Post Partum ComplicationDocument29 paginiPost Partum ComplicationPutri Rizky AmaliaÎncă nu există evaluări
- Seminar On Minor DisorderDocument23 paginiSeminar On Minor Disorderpriti pallabi100% (1)
- P ArtographDocument7 paginiP ArtographMali KanuÎncă nu există evaluări
- Charateristics of NewbornDocument3 paginiCharateristics of NewbornRagupathyRamanjuluÎncă nu există evaluări
- LabourDocument39 paginiLabourSravanthi Karingula100% (1)
- Multiple PregnancyDocument20 paginiMultiple PregnancyNurul Fahmiza TumiranÎncă nu există evaluări
- Prolonged Labor and Labor InductionDocument28 paginiProlonged Labor and Labor InductionNovia RizqiÎncă nu există evaluări
- Purperal InfectionsDocument69 paginiPurperal InfectionsBeulah DasariÎncă nu există evaluări
- Ectopic PregnancyDocument26 paginiEctopic PregnancysandhyakrishnanÎncă nu există evaluări
- Version FinalDocument22 paginiVersion FinalsanthiyasandyÎncă nu există evaluări
- Multiple Pregnancy: Presented byDocument49 paginiMultiple Pregnancy: Presented byvarshasharma05Încă nu există evaluări
- Multiple PregnancyDocument16 paginiMultiple Pregnancyjane7arian7berzabalÎncă nu există evaluări
- Seminar MenopauseDocument51 paginiSeminar MenopauseKelvin SuÎncă nu există evaluări
- Procedure Assignment For ManagementDocument7 paginiProcedure Assignment For ManagementPatel Amee100% (1)
- Physiology of LactationDocument3 paginiPhysiology of LactationAswathy Chandran100% (1)
- Ante Partum HemorrhageDocument30 paginiAnte Partum Hemorrhagetanmai nooluÎncă nu există evaluări
- Hyperemesis GravidarumDocument16 paginiHyperemesis GravidarumGracy Casaña100% (2)
- FEOTAL MEASURE Clinical ParametersDocument13 paginiFEOTAL MEASURE Clinical Parameterssuman guptaÎncă nu există evaluări
- Obstructed Labour (OL)Document34 paginiObstructed Labour (OL)ruhulcoc1Încă nu există evaluări
- Ob Seminar Amniotic Fluid-1Document25 paginiOb Seminar Amniotic Fluid-1Aleena Davis100% (1)
- Fetal Physiological Measurements: Proceedings of the Second International Conference on Fetal and Neonatal Physiological MeasurementsDe la EverandFetal Physiological Measurements: Proceedings of the Second International Conference on Fetal and Neonatal Physiological MeasurementsPeter RolfeÎncă nu există evaluări
- Instruction Manual in Obstetrics: Volume OneDe la EverandInstruction Manual in Obstetrics: Volume OneÎncă nu există evaluări
- 3 Use Thyroid Gland Use TTDocument55 pagini3 Use Thyroid Gland Use TTMathy MtenjeÎncă nu există evaluări
- 10 Nutrients To Improve Thyroid FunctionDocument21 pagini10 Nutrients To Improve Thyroid FunctionsiesmannÎncă nu există evaluări
- Hyperthyroidism in Pregnancy: Jorge H. MDDocument23 paginiHyperthyroidism in Pregnancy: Jorge H. MDRashid HussainÎncă nu există evaluări
- Diseases of Endocrine SystemDocument84 paginiDiseases of Endocrine SystemDuaa The PandaÎncă nu există evaluări
- Guidelines of The American Thyroid Association PREGNANCY PDFDocument47 paginiGuidelines of The American Thyroid Association PREGNANCY PDFIqra AnugerahÎncă nu există evaluări
- Obstetrics MCQ: Amanda Leow AFP NHS Lothian 20 Jan 2021Document62 paginiObstetrics MCQ: Amanda Leow AFP NHS Lothian 20 Jan 2021Amanda LeowÎncă nu există evaluări
- Hypothyroidism - Practice Essentials, Background, PathophysiologyDocument17 paginiHypothyroidism - Practice Essentials, Background, PathophysiologyprobowurÎncă nu există evaluări
- Thyroid Colloid Nodular GoiterDocument23 paginiThyroid Colloid Nodular Goitervahn025Încă nu există evaluări
- Summary of HyperthyroidismDocument8 paginiSummary of HyperthyroidismAbedinego MalukaÎncă nu există evaluări
- 1-Thyroid and Antithyroid Drugs (This)Document96 pagini1-Thyroid and Antithyroid Drugs (This)hamidÎncă nu există evaluări
- IEC Presentation PintuDocument25 paginiIEC Presentation PintuPintu MahtoÎncă nu există evaluări
- ENDOCRINE SYSTEM - REVIEWERDocument9 paginiENDOCRINE SYSTEM - REVIEWERVanya YeleniaÎncă nu există evaluări
- Down Syndrome Associated ComplicationsDocument3 paginiDown Syndrome Associated ComplicationsAlyssa Jean AlcoranÎncă nu există evaluări
- Nurul Nadia Noor Azlan - Syaza Izzati Zahari: Group 84Document52 paginiNurul Nadia Noor Azlan - Syaza Izzati Zahari: Group 84Nurul NadiaÎncă nu există evaluări
- MCQDocument21 paginiMCQNazaqat FarooqÎncă nu există evaluări
- Case StudyDocument4 paginiCase Studyllyryc100% (1)
- Thyroid DiseasesDocument5 paginiThyroid DiseasesSholehuddin MunajjidÎncă nu există evaluări
- (Endocrinology) Paolo Vitti, Laszlo Hegedus (Eds.) - Thyroid Diseases - Pathogenesis, Diagnosis and Treatment-Springer International Publishing PDFDocument478 pagini(Endocrinology) Paolo Vitti, Laszlo Hegedus (Eds.) - Thyroid Diseases - Pathogenesis, Diagnosis and Treatment-Springer International Publishing PDFOktahermoniza TanjungÎncă nu există evaluări
- Thyroid SolutionDocument58 paginiThyroid Solutionalbinuta100% (2)
- Thyroid DisordersDocument67 paginiThyroid DisordersMA 09Încă nu există evaluări
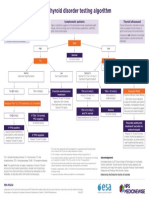
- NPS MedicineWise Thyroid Testing Algorithm v3Document1 paginăNPS MedicineWise Thyroid Testing Algorithm v3Mikhael JHÎncă nu există evaluări
- Drugs Affecting The Endocrine SystemDocument3 paginiDrugs Affecting The Endocrine SystemJerica Jaz F. VergaraÎncă nu există evaluări
- Tutorial On Goiter GadedDocument117 paginiTutorial On Goiter GadedhindabdalgadirÎncă nu există evaluări
- The Child With Endocrine DysfunctionDocument5 paginiThe Child With Endocrine Dysfunctionhenny1620Încă nu există evaluări
- 1987Document15 pagini1987hasnaÎncă nu există evaluări
- FUNDA0319Document11 paginiFUNDA0319Clarissa Guifaya50% (2)
- New Zealand Data Sheet: 1 Product NameDocument8 paginiNew Zealand Data Sheet: 1 Product NameAhmed Abd El HakimÎncă nu există evaluări
- Thyroid Function TestsDocument21 paginiThyroid Function TestsPraneeth TirumalasettyÎncă nu există evaluări
- Comlex Ii & Usmle Ii Cram Sheets - Gastroenterology Vitamins ObesityDocument31 paginiComlex Ii & Usmle Ii Cram Sheets - Gastroenterology Vitamins ObesitySolomon Seth Sallfors100% (1)