S-ar putea să vă placă și
- Febrile Seizure and EpilepsyDocument41 paginiFebrile Seizure and EpilepsyNurÎncă nu există evaluări
- Emergency in EntDocument44 paginiEmergency in EntNurÎncă nu există evaluări
- Anatomy and Physiology of NoseDocument29 paginiAnatomy and Physiology of NoseNur100% (1)
- Temporal Bone FracturesDocument21 paginiTemporal Bone FracturesNurÎncă nu există evaluări
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Anatomy of Bone and JointDocument48 paginiAnatomy of Bone and JointKamalia Bint MuhammadÎncă nu există evaluări
- Skull, Cranial Base, Facial BoneDocument4 paginiSkull, Cranial Base, Facial BoneAlyana AbrantesÎncă nu există evaluări
- NeuroVascular (NV) Holding PointsDocument2 paginiNeuroVascular (NV) Holding PointsHatem Farouk100% (1)
- Chapter 139 Anatomy of The Skull Base Temporal Bone External Ear and Middle Ear Larry G Duckert - CompressDocument12 paginiChapter 139 Anatomy of The Skull Base Temporal Bone External Ear and Middle Ear Larry G Duckert - CompressWudieÎncă nu există evaluări
- Fetal Skull: Badeea Seliem Soliman Assistant Prof. of Gynecology and Obstetrics Zagazig UniversityDocument107 paginiFetal Skull: Badeea Seliem Soliman Assistant Prof. of Gynecology and Obstetrics Zagazig UniversityBharat Thapa50% (2)
- CRANIOVETEBRALJUNCTIONDocument130 paginiCRANIOVETEBRALJUNCTIONdrarunrao100% (1)
- ZOO3731 chptr.6-8Document55 paginiZOO3731 chptr.6-8Raylax2sik24Încă nu există evaluări
- Bio 201 - Bone Practical Part 1 (Axial Skeleton)Document5 paginiBio 201 - Bone Practical Part 1 (Axial Skeleton)Gretchen100% (1)
- Anatomy Tables-Arteries of The Head and NeckDocument20 paginiAnatomy Tables-Arteries of The Head and NeckTracie YWÎncă nu există evaluări
- OMM Fellows ReviewDocument178 paginiOMM Fellows ReviewTony Ziherl100% (1)
- Neuroanatomy Revision Notes PDFDocument7 paginiNeuroanatomy Revision Notes PDFTanya Tanu100% (1)
- Bone SkullDocument80 paginiBone SkullKumarÎncă nu există evaluări
- Anterior and Posterior Petrosectomy Seminar 13 Jan 2021 DR Abhinav 2Document76 paginiAnterior and Posterior Petrosectomy Seminar 13 Jan 2021 DR Abhinav 2Tamajyoti GhoshÎncă nu există evaluări
- Age EstimationDocument74 paginiAge EstimationMu'taz ArmanÎncă nu există evaluări
- Cat SkeletonDocument10 paginiCat SkeletonJefferson TanÎncă nu există evaluări
- Unilateral Greater Occipital Nerve Compression Causing Scalp NumbnessDocument2 paginiUnilateral Greater Occipital Nerve Compression Causing Scalp NumbnessIzzati N. SariÎncă nu există evaluări
- Skull Anatomy PDFDocument12 paginiSkull Anatomy PDFSiva Shanmugam100% (2)
- Motion Palpation Neil Davies PART 1Document9 paginiMotion Palpation Neil Davies PART 1Scott JacksonÎncă nu există evaluări
- Nie 2005Document9 paginiNie 2005Claypella MaskÎncă nu există evaluări
- Regenesis 1Document14 paginiRegenesis 1White Light100% (3)
- Endoskeleton of The ChickenDocument20 paginiEndoskeleton of The ChickenJoachimÎncă nu există evaluări
- Chiropractic Green Books - V09 - 1923Document582 paginiChiropractic Green Books - V09 - 1923Fabio DiasÎncă nu există evaluări
- Schaaffhausen 1858Document12 paginiSchaaffhausen 1858Anth5334Încă nu există evaluări
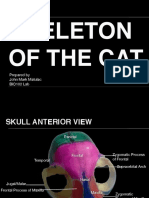
- Skeleton of The Cat: Prepared by John Mark Matulac BIO102 LabDocument27 paginiSkeleton of The Cat: Prepared by John Mark Matulac BIO102 LabJoachimÎncă nu există evaluări
- 8 WHO Standard Acupuncture Point Locations in The Westernpart 8Document32 pagini8 WHO Standard Acupuncture Point Locations in The Westernpart 8Virgil AnmaÎncă nu există evaluări
- MICRO TEACHING Physical Examination of ChildrenDocument5 paginiMICRO TEACHING Physical Examination of ChildrenSAGAR ADHAO100% (1)
- Nonsyndromic CraniosynostosisDocument10 paginiNonsyndromic CraniosynostosisOWintero OWarmoÎncă nu există evaluări
- Anatomy SharkDocument32 paginiAnatomy SharkKanwal RashidÎncă nu există evaluări
- Cunninghams Manual of Practical Anatomy 1000740114Document580 paginiCunninghams Manual of Practical Anatomy 1000740114adiseif100% (3)
- Skull Base PDFDocument106 paginiSkull Base PDFmalex33yÎncă nu există evaluări