S-ar putea să vă placă și
- Consultation-Liaison Psychiatry: Leslie M. Forman, M.D., Neil Scheurich, M.D., and Kristen Tyszkowski, M.DDocument45 paginiConsultation-Liaison Psychiatry: Leslie M. Forman, M.D., Neil Scheurich, M.D., and Kristen Tyszkowski, M.DRayanÎncă nu există evaluări
- Asia Map AtlasDocument1 paginăAsia Map AtlasCosmin MaresiÎncă nu există evaluări
- Approach To The Patient With Ongoing BleedingDocument2 paginiApproach To The Patient With Ongoing BleedingRayanÎncă nu există evaluări
- Epidemiology of Surgical Site InfectionDocument2 paginiEpidemiology of Surgical Site InfectionRayanÎncă nu există evaluări
- Anaemia'sDocument27 paginiAnaemia'sRayan100% (2)
- Breast CancerDocument69 paginiBreast CancerRayanÎncă nu există evaluări
- How To Find Lost Objects (1993-2008)Document67 paginiHow To Find Lost Objects (1993-2008)piliviu100% (1)
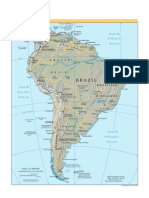
- CIA - World Factbook - Reference Map - South AmericaDocument1 paginăCIA - World Factbook - Reference Map - South Americaabhii100% (1)
- Initial Management of MalnutritionDocument2 paginiInitial Management of MalnutritionRayanÎncă nu există evaluări
- Mapa Mundi FisicoDocument1 paginăMapa Mundi FisicoMauricio Lopes AmorimÎncă nu există evaluări
- Maps of The World - North AmericaDocument1 paginăMaps of The World - North AmericaeternalravenÎncă nu există evaluări
- CIA - World Factbook - Reference Map - AntarcticDocument1 paginăCIA - World Factbook - Reference Map - AntarcticabhiiÎncă nu există evaluări
- CIA - World Factbook - Reference Map - OceaniaDocument1 paginăCIA - World Factbook - Reference Map - Oceaniaabhii100% (4)
- CIA - World Factbook - Reference Map - Europe KosovoDocument1 paginăCIA - World Factbook - Reference Map - Europe Kosovoabhii100% (1)
- CIA - World Factbook - Reference Map - Central AmericaDocument1 paginăCIA - World Factbook - Reference Map - Central AmericaabhiiÎncă nu există evaluări
- Mapa Mundi PolíticoDocument1 paginăMapa Mundi PolíticoRuan MüllerÎncă nu există evaluări
- Atlante - Middle EastDocument1 paginăAtlante - Middle EastTiziano MazzoleniÎncă nu există evaluări
- CIA - World Factbook - Reference Map - ArcticDocument1 paginăCIA - World Factbook - Reference Map - Arcticabhii100% (1)
- Asia PDFDocument1 paginăAsia PDFFreakbizarroÎncă nu există evaluări
- MalariaDocument34 paginiMalariaRayanÎncă nu există evaluări
- CIA - World Factbook - Reference Map - Time ZonesDocument1 paginăCIA - World Factbook - Reference Map - Time Zonesabhii100% (2)
- Maps of The World - AfricaDocument1 paginăMaps of The World - AfricaDanielÎncă nu există evaluări
- Evalutaion of Abdominal TraumaDocument1 paginăEvalutaion of Abdominal TraumaRayanÎncă nu există evaluări
- Xrays & CTsDocument30 paginiXrays & CTsRayan100% (1)
- Leishmanisis in Sudan: A Literature Review With Emphasis On Clinical AspectsDocument7 paginiLeishmanisis in Sudan: A Literature Review With Emphasis On Clinical AspectsRayan100% (1)
- Visceral Leishmaniasis: Current Status of Control, Diagnosis, and Treatment, and A Proposed Research and Development AgendaDocument8 paginiVisceral Leishmaniasis: Current Status of Control, Diagnosis, and Treatment, and A Proposed Research and Development AgendaRayan100% (2)
- History Taking PrinciplesDocument1 paginăHistory Taking PrinciplesRayan100% (1)
- The Amazing Quran by Gary MillerDocument17 paginiThe Amazing Quran by Gary MillerRayan50% (2)
- Chocolate Fantasy 20 RecipesDocument22 paginiChocolate Fantasy 20 RecipesRayanÎncă nu există evaluări
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- AMU BALLB (Hons.) 2018 SyllabusDocument13 paginiAMU BALLB (Hons.) 2018 SyllabusA y u s hÎncă nu există evaluări
- Productflyer - 978 1 4020 5716 8Document1 paginăProductflyer - 978 1 4020 5716 8jmendozaqÎncă nu există evaluări
- Rincian Kewenangan Klinis AnakDocument6 paginiRincian Kewenangan Klinis AnakUchiha ItachiÎncă nu există evaluări
- My Pitch p2Document16 paginiMy Pitch p2api-477556951Încă nu există evaluări
- Mech302hw5s 2Document11 paginiMech302hw5s 2priyadarshini212007Încă nu există evaluări
- Use of ICT in School AdministartionDocument32 paginiUse of ICT in School AdministartionSyed Ali Haider100% (1)
- Lesson Plan in Explicirt Teaching in Oral Lnguage and Grammar (Checked)Document3 paginiLesson Plan in Explicirt Teaching in Oral Lnguage and Grammar (Checked)Lovella GacaÎncă nu există evaluări
- EmanDocument3 paginiEmanCh NawazÎncă nu există evaluări
- Travel Smart: Assignment 1: Project ProposalDocument14 paginiTravel Smart: Assignment 1: Project ProposalcattytomeÎncă nu există evaluări
- CH 2 & CH 3 John R. Schermerhorn - Management-Wiley (2020)Document9 paginiCH 2 & CH 3 John R. Schermerhorn - Management-Wiley (2020)Muhammad Fariz IbrahimÎncă nu există evaluări
- 208 C - Algebras: Marc Rieffel Notes by Qiaochu Yuan Spring 2013Document55 pagini208 C - Algebras: Marc Rieffel Notes by Qiaochu Yuan Spring 2013Nikos AthanasiouÎncă nu există evaluări
- Sonnet WorksheetDocument3 paginiSonnet WorksheetMary Cris EspirituÎncă nu există evaluări
- Heart Rate Variability - Wikipedia PDFDocument30 paginiHeart Rate Variability - Wikipedia PDFLevon HovhannisyanÎncă nu există evaluări
- Appendix I Leadership Questionnaire: Ior Description Questionnaire (LBDQ - Form XII 1962) - The Division IntoDocument24 paginiAppendix I Leadership Questionnaire: Ior Description Questionnaire (LBDQ - Form XII 1962) - The Division IntoJoan GonzalesÎncă nu există evaluări
- EC SF Presentation 02Document10 paginiEC SF Presentation 02Ahmed NafeaÎncă nu există evaluări
- MathTextbooks9 12Document64 paginiMathTextbooks9 12Andrew0% (1)
- Public Service: P2245m-PorkDocument3 paginiPublic Service: P2245m-PorkDaniela Ellang ManuelÎncă nu există evaluări
- Blue Mountain Coffee Case (ADBUDG)Document16 paginiBlue Mountain Coffee Case (ADBUDG)Nuria Sánchez Celemín100% (1)
- HR Recruiter Interview Question & AnswerDocument6 paginiHR Recruiter Interview Question & AnswerGurukrushna PatnaikÎncă nu există evaluări
- Accounting TheoryDocument192 paginiAccounting TheoryABDULLAH MOHAMMEDÎncă nu există evaluări
- MidtermDocument8 paginiMidtermBrian FrenchÎncă nu există evaluări
- Nutrition and Diet Therapy ExaminationDocument8 paginiNutrition and Diet Therapy ExaminationIrwan M. Iskober100% (3)
- Dollar Unit SamplingDocument7 paginiDollar Unit SamplingAndriatsirihasinaÎncă nu există evaluări
- ABC of Effective WritingDocument4 paginiABC of Effective Writingprada85Încă nu există evaluări
- Normalization Techniques For Multi-Criteria Decision Making: Analytical Hierarchy Process Case StudyDocument11 paginiNormalization Techniques For Multi-Criteria Decision Making: Analytical Hierarchy Process Case StudyJohn GreenÎncă nu există evaluări
- Reflection (The We Entrepreneur)Document2 paginiReflection (The We Entrepreneur)Marklein DumangengÎncă nu există evaluări
- Aleister Crowley Astrological Chart - A Service For Members of Our GroupDocument22 paginiAleister Crowley Astrological Chart - A Service For Members of Our GroupMysticalgod Uidet100% (3)
- 2009-Journal of Pharmacy and PharmacologyDocument37 pagini2009-Journal of Pharmacy and PharmacologyLeticia Bonancio CerqueiraÎncă nu există evaluări
- Post-Stroke Rehabilitation: Kazan State Medical UniversityDocument11 paginiPost-Stroke Rehabilitation: Kazan State Medical UniversityAigulÎncă nu există evaluări
- Baath Arab Socialist Party - Constitution (Approved in 1947)Document9 paginiBaath Arab Socialist Party - Constitution (Approved in 1947)Antonio de OdilonÎncă nu există evaluări