S-ar putea să vă placă și
- Lactic Acidosis Update For Critical Care CliniciansDocument5 paginiLactic Acidosis Update For Critical Care CliniciansjohjossÎncă nu există evaluări
- Rapid Sequence Intubation: BY Budak KecikDocument25 paginiRapid Sequence Intubation: BY Budak KecikAqua ForceÎncă nu există evaluări
- Sepsis Update 2018Document32 paginiSepsis Update 2018putri endah100% (1)
- 10 1001@jama 2016 0287Document10 pagini10 1001@jama 2016 0287ompardor7554Încă nu există evaluări
- ContohDocument4 paginiContohAqua ForceÎncă nu există evaluări
- Prevention Cardio CPGDocument63 paginiPrevention Cardio CPGAqua ForceÎncă nu există evaluări
- Rapid Sequence Intubation: BY Budak KecikDocument25 paginiRapid Sequence Intubation: BY Budak KecikAqua ForceÎncă nu există evaluări
- Preterm Labor DahliaDocument4 paginiPreterm Labor DahliaAqua ForceÎncă nu există evaluări
- Senarai Ho Banjir Medical 2014 PDFDocument4 paginiSenarai Ho Banjir Medical 2014 PDFAqua ForceÎncă nu există evaluări
- Att Letters SecDocument6 paginiAtt Letters SecAqua ForceÎncă nu există evaluări
- CampioneDocument1.652 paginiCampioneAqua ForceÎncă nu există evaluări
- ReadmeDocument7 paginiReadmeLambourghiniÎncă nu există evaluări
- Absenteeism Letter On Letterhead PDFDocument2 paginiAbsenteeism Letter On Letterhead PDFAqua ForceÎncă nu există evaluări
- DfsdfsdfeerberwerberbwerweDocument1 paginăDfsdfsdfeerberwerberbwerweAqua ForceÎncă nu există evaluări
- NRDSDocument4 paginiNRDSAqua ForceÎncă nu există evaluări
- UK National Guideline For The Management of Pelvic Inflammatory Disease 2011 PDFDocument18 paginiUK National Guideline For The Management of Pelvic Inflammatory Disease 2011 PDFPrissilmaTaniaÎncă nu există evaluări
- VDFHGFHF Rtretr GR Df33254Document1 paginăVDFHGFHF Rtretr GR Df33254Aqua ForceÎncă nu există evaluări
- Coordinator of Six Year Prof Dr/Ahmed TarekDocument1 paginăCoordinator of Six Year Prof Dr/Ahmed TarekAqua ForceÎncă nu există evaluări
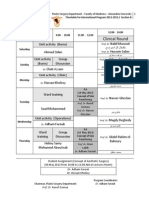
- Timetable For International Program 2012-2013 - Section BDocument1 paginăTimetable For International Program 2012-2013 - Section BAqua ForceÎncă nu există evaluări
- Emergency HTNDocument6 paginiEmergency HTNAqua ForceÎncă nu există evaluări
- Approach To Chest PainDocument17 paginiApproach To Chest PainAqua ForceÎncă nu există evaluări
- Torrent Downloaded FromDocument1 paginăTorrent Downloaded FromAqua ForceÎncă nu există evaluări
- Ent Past Years Question According To TopicsDocument32 paginiEnt Past Years Question According To Topicsmohamed100% (1)
- 243ear TraumaDocument33 pagini243ear TraumaAqua ForceÎncă nu există evaluări
- Examples of OSCEDocument2 paginiExamples of OSCEAqua ForceÎncă nu există evaluări
- Examples of OSCEDocument2 paginiExamples of OSCEAqua ForceÎncă nu există evaluări
- Management of Head InjuriesDocument8 paginiManagement of Head InjuriesAqua ForceÎncă nu există evaluări
- Surgery TopicsDocument1 paginăSurgery TopicsAqua ForceÎncă nu există evaluări
- Autoimmune Bullous DermatosesDocument143 paginiAutoimmune Bullous DermatosesAqua ForceÎncă nu există evaluări
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Aim-120 Amraam: Advanced Medium Range Air-to-Air MissileDocument10 paginiAim-120 Amraam: Advanced Medium Range Air-to-Air MissileA RozzÎncă nu există evaluări
- A2szs9ffwesiretp8j0mwchwpkmk3hmako6c5ivo (3) 1 4Document18 paginiA2szs9ffwesiretp8j0mwchwpkmk3hmako6c5ivo (3) 1 4Heidi Ferrari Schafer de AndradeÎncă nu există evaluări
- PEOPLE OF THE PHILIPPINES vs. VICTOR TANEODocument4 paginiPEOPLE OF THE PHILIPPINES vs. VICTOR TANEOSarah Monique Nicole Antoinette GolezÎncă nu există evaluări
- Script - The RunawayDocument9 paginiScript - The Runawayapi-461261491Încă nu există evaluări
- Topic TDC15!01!004 - Driver's License SystemDocument6 paginiTopic TDC15!01!004 - Driver's License SystemDranej Fang PobÎncă nu există evaluări
- Pending PMOPG E 2017 0264525 5 5 17Document1 paginăPending PMOPG E 2017 0264525 5 5 17Anonymous n4UccmT6qÎncă nu există evaluări
- Founding Affidavit Part 1 Without Annexures Mutaambanda KapikaDocument29 paginiFounding Affidavit Part 1 Without Annexures Mutaambanda KapikaStrandwolfÎncă nu există evaluări
- Prologue Magazine - Winter 2008 - Vol. 40, No. 4Document76 paginiPrologue Magazine - Winter 2008 - Vol. 40, No. 4Prologue Magazine100% (1)
- Working Hours & AttendanceDocument6 paginiWorking Hours & AttendancesupriyaÎncă nu există evaluări
- Valour-IT July 2012Document2 paginiValour-IT July 2012Doug WelchÎncă nu există evaluări
- Biographical Sketch For Students Format Solved Examples Worksheet PDFDocument6 paginiBiographical Sketch For Students Format Solved Examples Worksheet PDFAyush NayakÎncă nu există evaluări
- Jordan Trademark Case: IssueDocument3 paginiJordan Trademark Case: IssueKeisya Naomi NababanÎncă nu există evaluări
- Harry PotterDocument14 paginiHarry PotterRahul100% (3)
- Respondent Memorial FinalDocument21 paginiRespondent Memorial FinalIM-23 S1Încă nu există evaluări
- (Sec 9-14) Ali, Hanifa ShereenDocument20 pagini(Sec 9-14) Ali, Hanifa ShereenHanifa Shereen Biston AliÎncă nu există evaluări
- 1 - The Barn at The End of Our Term - Granta 97 - Best of Young American Novelists 2 - Archive - Granta MagazineDocument15 pagini1 - The Barn at The End of Our Term - Granta 97 - Best of Young American Novelists 2 - Archive - Granta MagazineabujeiÎncă nu există evaluări
- Suffrage (Art. V)Document10 paginiSuffrage (Art. V)alfieÎncă nu există evaluări
- Law Case StudyDocument2 paginiLaw Case StudyRafia ShabbirÎncă nu există evaluări
- G0956Document84 paginiG0956sedattasyurek100% (3)
- Must (Be) Can'T (Be) Present Probable May (Be) May Not (Be) Might (Be) Might Not (Be)Document4 paginiMust (Be) Can'T (Be) Present Probable May (Be) May Not (Be) Might (Be) Might Not (Be)Guadalupe Elizabeth Alvarez Lopez100% (1)
- Prelims 2009 GS KeyDocument26 paginiPrelims 2009 GS Keysatish kumarÎncă nu există evaluări
- C. B. WILLIAMS v. JOSE McMICKING G.R. No. L-6079 December 6, 1910 PDFDocument5 paginiC. B. WILLIAMS v. JOSE McMICKING G.R. No. L-6079 December 6, 1910 PDFZack SeiferÎncă nu există evaluări
- Romanian PTSD - Articol OnlineDocument33 paginiRomanian PTSD - Articol Onlineavram christianaÎncă nu există evaluări
- Corpo Cases Analytic Memo 2Document47 paginiCorpo Cases Analytic Memo 2jane ling adolfoÎncă nu există evaluări
- Copia de Reported Speech1Document2 paginiCopia de Reported Speech1L�PEZ COTERILLO MART�NÎncă nu există evaluări
- GEC 9 Reaction Paper 2Document2 paginiGEC 9 Reaction Paper 2Cristal Cielo MarzanÎncă nu există evaluări
- Board of Assessment Appeals vs. Manila Electric Co.: Presented By: Cuento, Joshua T. Jd2-PropertyDocument9 paginiBoard of Assessment Appeals vs. Manila Electric Co.: Presented By: Cuento, Joshua T. Jd2-PropertyJoshua CuentoÎncă nu există evaluări
- A. They Took No Notice of ItDocument4 paginiA. They Took No Notice of ItNicolas Santiago Orozco Arias 1105Încă nu există evaluări
- Cundy Smith Civil Litigation Law School PDFDocument347 paginiCundy Smith Civil Litigation Law School PDFFAJECS Intl100% (1)
- Secretary-Certificate LetterDocument2 paginiSecretary-Certificate Letterteresa bautistaÎncă nu există evaluări