S-ar putea să vă placă și
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Step 2 NotesDocument202 paginiStep 2 NotesNaved Rahman100% (2)
- Epn 2 Modul 1Document3 paginiEpn 2 Modul 1Ary FahrizanÎncă nu există evaluări
- Pathology Laboratory in AhmedabadDocument73 paginiPathology Laboratory in Ahmedabaddivyesh_sharma_20% (1)
- Facts and Definition of EclampsiaDocument5 paginiFacts and Definition of EclampsiaChoi Gong JuÎncă nu există evaluări
- Obstetric FistulaDocument8 paginiObstetric FistulaHyderabad hhcÎncă nu există evaluări
- VulvovaginiteDocument17 paginiVulvovaginiteAndreea DanielaÎncă nu există evaluări
- Butuan Doctors' College: O.R. Scrub Form MajorDocument4 paginiButuan Doctors' College: O.R. Scrub Form MajorNheljane DelacruzÎncă nu există evaluări
- Investigation Seminar: Urine Pregnancy TestDocument29 paginiInvestigation Seminar: Urine Pregnancy TestDr ajayÎncă nu există evaluări
- Pocket-Book MCH Emergencies - English PDFDocument286 paginiPocket-Book MCH Emergencies - English PDFAbigail Kusi-Amponsah100% (1)
- Department Check List Final 3Document27 paginiDepartment Check List Final 3BOOKREADER_NOWÎncă nu există evaluări
- Obstetrics HistoryDocument3 paginiObstetrics HistorymakepaÎncă nu există evaluări
- Ardo Master PDFDocument24 paginiArdo Master PDFNurhidayah AyuÎncă nu există evaluări
- Effect of Foot Massage To Decrease Physiological Lower Leg Oedema in Late Pregnancy: A Randomized Controlled Trial in TurkeyDocument7 paginiEffect of Foot Massage To Decrease Physiological Lower Leg Oedema in Late Pregnancy: A Randomized Controlled Trial in TurkeyRichaanggrainiÎncă nu există evaluări
- Placenta IsuogDocument40 paginiPlacenta IsuogKARINA BASTIDAS IBARRA100% (1)
- Wikipedia - Adams-Stokes Syndrome (CHECKED)Document2 paginiWikipedia - Adams-Stokes Syndrome (CHECKED)pixoguiasÎncă nu există evaluări
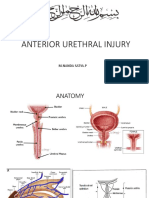
- Rupture Urethra Anterior DR Sule FixDocument36 paginiRupture Urethra Anterior DR Sule FixkadinfathiaÎncă nu există evaluări
- YASASII - Nursing ManualDocument20 paginiYASASII - Nursing ManualSalma Alsheikh AbdullahÎncă nu există evaluări
- CullpDocument3 paginiCullpGulherme NodaÎncă nu există evaluări
- FaicoDocument3 paginiFaicoknbabuÎncă nu există evaluări
- Neoplasma UterineDocument102 paginiNeoplasma UterineAlifa Nasyahta RosianaÎncă nu există evaluări
- Maxillary Transverse DeficiencyDocument4 paginiMaxillary Transverse DeficiencyCarlos Alberto CastañedaÎncă nu există evaluări
- SEMINAR ON MULTIPLE PREGNANCY ContentDocument21 paginiSEMINAR ON MULTIPLE PREGNANCY ContentMonika shankar0% (1)
- Radial Nerve InjuryDocument5 paginiRadial Nerve InjuryMuhammad RezaÎncă nu există evaluări
- The Menstrual Cycle ForDocument4 paginiThe Menstrual Cycle ForAngelica Calamba CalicaÎncă nu există evaluări
- Medical Surgical Nursing PDFDocument24 paginiMedical Surgical Nursing PDFRuhi PardhiÎncă nu există evaluări
- Disseminated Intravascular Coagulation (DIC) During Pregnancy - Clinical Findings, Etiology, and Diagnosis - UpToDateDocument23 paginiDisseminated Intravascular Coagulation (DIC) During Pregnancy - Clinical Findings, Etiology, and Diagnosis - UpToDateCristinaCaprosÎncă nu există evaluări
- Health Information System Developmen T (Medical Records)Document21 paginiHealth Information System Developmen T (Medical Records)skidz137217100% (10)
- EAACI - Food Allergy and Anaphylaxi PDFDocument294 paginiEAACI - Food Allergy and Anaphylaxi PDFoci savitrieÎncă nu există evaluări
- Patient Monitoring1370Document53 paginiPatient Monitoring1370Ridha Surya NugrahaÎncă nu există evaluări
- Filed Under: Multifocal Atrial TachycardiaDocument3 paginiFiled Under: Multifocal Atrial TachycardiaBogdan TeoÎncă nu există evaluări