S-ar putea să vă placă și
- Anaerobic Infections in HumansDe la EverandAnaerobic Infections in HumansSydney FinegoldEvaluare: 5 din 5 stele5/5 (1)
- Stroke: Kamau, Joy W. Med ViDocument88 paginiStroke: Kamau, Joy W. Med ViJoy Kamau100% (1)
- Stroke 1Document1 paginăStroke 1Trisha VergaraÎncă nu există evaluări
- Gastrointestinal System: Chapter EighteenDocument32 paginiGastrointestinal System: Chapter Eighteenhayascent hilarioÎncă nu există evaluări
- Intracranial Hypertension or Increased ICPDocument11 paginiIntracranial Hypertension or Increased ICPRomina Irish MatutinoÎncă nu există evaluări
- Cerebrovascular AccidentDocument79 paginiCerebrovascular AccidentKathy B. AbuanÎncă nu există evaluări
- Coma Dfiferential DiagnosisDocument23 paginiComa Dfiferential DiagnosisGeorge GeorgeÎncă nu există evaluări
- Subdural HematomaDocument8 paginiSubdural HematomaaaronmanullangÎncă nu există evaluări
- Guidelines For The Management of Severe Traumatic Brain Injury 4th EditionDocument62 paginiGuidelines For The Management of Severe Traumatic Brain Injury 4th EditionNailahRahmahÎncă nu există evaluări
- Traumatic Brain Injury: Dan Sprando Andres TabaresDocument31 paginiTraumatic Brain Injury: Dan Sprando Andres Tabaresanony7546 pop100% (1)
- Focus On StrokeDocument92 paginiFocus On StrokeDIAH RETNO WULAN100% (2)
- Ix StrokeDocument6 paginiIx StrokeWayne MacrohonÎncă nu există evaluări
- Health Questionnaire CandidateDocument5 paginiHealth Questionnaire CandidateSaudia Arabia JobsÎncă nu există evaluări
- Traumatic Brain InjuryDocument88 paginiTraumatic Brain Injurympm8471Încă nu există evaluări
- Types of Skull FractureDocument5 paginiTypes of Skull FractureKhor Hui DiÎncă nu există evaluări
- Head TraumaDocument15 paginiHead TraumaDede Yusuf FÎncă nu există evaluări
- AneurysmDocument22 paginiAneurysmJeremiash Noblesala Dela CruzÎncă nu există evaluări
- Alzheimeru2019s DiseaseDocument17 paginiAlzheimeru2019s Diseaseapi-262538456100% (1)
- Neurologic Assessment Physiologic Changes With AgingDocument4 paginiNeurologic Assessment Physiologic Changes With AgingDarl Dacdac100% (1)
- Whipple Procedure: (Pancreaticoduodenectomy)Document13 paginiWhipple Procedure: (Pancreaticoduodenectomy)gamaÎncă nu există evaluări
- Head Injury Classification: Head Injuries/Head Trauma 1 - Closed (Blunt) Brain InjuryDocument4 paginiHead Injury Classification: Head Injuries/Head Trauma 1 - Closed (Blunt) Brain InjuryClarisse Biagtan CerameÎncă nu există evaluări
- Parkinson's DiseaseDocument52 paginiParkinson's Diseasealolika dolaiÎncă nu există evaluări
- Pediatric Brain TumorsDocument19 paginiPediatric Brain TumorsTezza DinayantiÎncă nu există evaluări
- Cerebral Concussion - PathophyDocument6 paginiCerebral Concussion - PathophyFretzgine Lou Manuel100% (1)
- Degenerative Neurological DisordersDocument61 paginiDegenerative Neurological DisordersMarites Santos AquinoÎncă nu există evaluări
- Journal - Alzheimer DiseaseDocument1 paginăJournal - Alzheimer DiseaseTriLightÎncă nu există evaluări
- 1228 HFStroke Altered Neuro 2011Document74 pagini1228 HFStroke Altered Neuro 2011Cyndy EnterlineÎncă nu există evaluări
- W3 - MEDSURG Neurologic Disorders (MS, MG, and Parkisons's)Document11 paginiW3 - MEDSURG Neurologic Disorders (MS, MG, and Parkisons's)Kyla L. MadjadÎncă nu există evaluări
- Elimination Disorder: Presented by Saba AhmedDocument49 paginiElimination Disorder: Presented by Saba AhmedRana Ahmad Gulraiz100% (1)
- Cerebro Vascular AccidentDocument82 paginiCerebro Vascular AccidentJayvee Novenario Casaljay100% (1)
- Part 3 Huntingtons To EpilepsyDocument10 paginiPart 3 Huntingtons To EpilepsyNurse Ambassadors100% (1)
- Cerebrovascular AccidentDocument62 paginiCerebrovascular AccidentJaydee DalayÎncă nu există evaluări
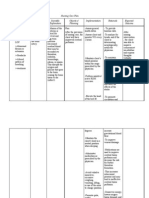
- Nursing Care Plan: Assessment Diagnosis Inference Planning Intervention Rationale EvaluationDocument3 paginiNursing Care Plan: Assessment Diagnosis Inference Planning Intervention Rationale EvaluationJessa FabicoÎncă nu există evaluări
- Cell Ab Midterm MesiDocument7 paginiCell Ab Midterm MesiSamantha VeraÎncă nu există evaluări
- Head Trauma & Management: Dr. Utham Murali. M.S M.B.A. Asso - Prof of Surgery IMS / MSU / MalaysiaDocument48 paginiHead Trauma & Management: Dr. Utham Murali. M.S M.B.A. Asso - Prof of Surgery IMS / MSU / MalaysiaNinaÎncă nu există evaluări
- w4 - Medsurg Brain Injury and SciDocument13 paginiw4 - Medsurg Brain Injury and SciKyla L. Madjad100% (1)
- Ischemic Stroke: The Normal Blood Supply To The Brain Is DisruptedDocument5 paginiIschemic Stroke: The Normal Blood Supply To The Brain Is DisruptedMelchora Lea Castro SorianoÎncă nu există evaluări
- Head & Brain Trauma: EMS Professions Temple CollegeDocument77 paginiHead & Brain Trauma: EMS Professions Temple CollegeElvan Dwi WidyadiÎncă nu există evaluări
- 01 Intro Pcol-MergedDocument19 pagini01 Intro Pcol-MergedlumpiaÎncă nu există evaluări
- Brain Attack: StrokeDocument49 paginiBrain Attack: Strokeceudmd3d100% (1)
- Approach To Unconsious PTDocument62 paginiApproach To Unconsious PTHussain AzharÎncă nu există evaluări
- Infectious Disease Awareness In, Mogadishu, SomaliaDocument7 paginiInfectious Disease Awareness In, Mogadishu, Somaliashafie Mohamed AliÎncă nu există evaluări
- Head, Mouth, Nose, Throat, Neck and Regional Lymph Nodes: Kristin Clephane, MSN, RN, CPNDocument44 paginiHead, Mouth, Nose, Throat, Neck and Regional Lymph Nodes: Kristin Clephane, MSN, RN, CPNMike100% (1)
- Head Injury Outline of Management CDocument89 paginiHead Injury Outline of Management CPanna SahaÎncă nu există evaluări
- Common Eye DiseasesDocument54 paginiCommon Eye Diseaseskyro draxÎncă nu există evaluări
- REVISED Head InjuryDocument4 paginiREVISED Head InjuryJanselle H Arma0% (1)
- Multiple SclerosisDocument6 paginiMultiple SclerosisRonnel Alvin Antonio AdrianoÎncă nu există evaluări
- Brain Injury Aftr Head Trauma Pathophysiology Diagnosis and TreatmentDocument18 paginiBrain Injury Aftr Head Trauma Pathophysiology Diagnosis and TreatmentMarcela SolarteÎncă nu există evaluări
- W2 - MEDSURG Guidelines For Nursing Interventions On Coma PatientsDocument6 paginiW2 - MEDSURG Guidelines For Nursing Interventions On Coma PatientsKyla L. Madjad100% (1)
- Cranial NervesDocument14 paginiCranial NervesIrina Garlea-Robu100% (1)
- List of Cranial NervesDocument2 paginiList of Cranial NervesKay Lumpas Cruda100% (1)
- Head Injury 2Document47 paginiHead Injury 2drvishal bhattÎncă nu există evaluări
- Neurologic EmergenciesDocument194 paginiNeurologic Emergenciesapi-205902640Încă nu există evaluări
- Moca Vs MMSEDocument2 paginiMoca Vs MMSEYw LiuÎncă nu există evaluări
- Epidural Hematoma: Kurniasari Armayana AhmadDocument10 paginiEpidural Hematoma: Kurniasari Armayana AhmadSuci AlimaÎncă nu există evaluări
- Neurologic DiseasesDocument13 paginiNeurologic DiseasesCzarinah BacuadoÎncă nu există evaluări
- MS Neurologic Conditions J2018 Ans KeyDocument13 paginiMS Neurologic Conditions J2018 Ans KeyPaul Lexus Gomez LorenzoÎncă nu există evaluări
- Marking Key Head InjuryDocument8 paginiMarking Key Head Injurymatildahkasakula492Încă nu există evaluări
- CVA-NCPDocument7 paginiCVA-NCPAiza Oronce0% (1)
- 1 Final Bedsidemngtofpt 190213111618 1Document17 pagini1 Final Bedsidemngtofpt 190213111618 1Chirag ParmarÎncă nu există evaluări
- Course No.: BIOF216 Course Title: Water, Sanitation and Solid Waste ManagementDocument6 paginiCourse No.: BIOF216 Course Title: Water, Sanitation and Solid Waste ManagementJeswin EldhoÎncă nu există evaluări
- Treating The Mother of Black Triangles With Bioclear VeneersDocument4 paginiTreating The Mother of Black Triangles With Bioclear VeneersThe Bioclear ClinicÎncă nu există evaluări
- CRFDocument27 paginiCRFNatalie WÎncă nu există evaluări
- Futuristic NursingDocument3 paginiFuturistic NursingDeerpraj CmÎncă nu există evaluări
- Psychosexual Stages and Defense MechanismsDocument20 paginiPsychosexual Stages and Defense MechanismsJia V JÎncă nu există evaluări
- The Vodka Diet Edit 12.20Document114 paginiThe Vodka Diet Edit 12.20Late Knight GamingÎncă nu există evaluări
- Drug Study - CaDocument3 paginiDrug Study - Casaint_ronald8Încă nu există evaluări
- Four Square Step TestDocument2 paginiFour Square Step TestAnonymous igISmSUÎncă nu există evaluări
- FST 225Document63 paginiFST 225Karthikeyan BalakrishnanÎncă nu există evaluări
- Goat MilkDocument39 paginiGoat Milkinkpen56789Încă nu există evaluări
- Endo Morphology Chart PDFDocument1 paginăEndo Morphology Chart PDFNaji Z. ArandiÎncă nu există evaluări
- Aapm TG 25Document40 paginiAapm TG 25AnjihartsÎncă nu există evaluări
- Resident Medical Officer KAmL4W116erDocument4 paginiResident Medical Officer KAmL4W116erAman TyagiÎncă nu există evaluări
- Mada Murch SanyasaDocument27 paginiMada Murch SanyasaKs manjunatha78% (9)
- Sterilization of Water Using Bleaching Powder: A Chemistry Investigatory ProjectDocument21 paginiSterilization of Water Using Bleaching Powder: A Chemistry Investigatory ProjectIshan thakurÎncă nu există evaluări
- Five To 10-Year Followup of Open Partial Nephrectomy in A Solitary KidneyDocument5 paginiFive To 10-Year Followup of Open Partial Nephrectomy in A Solitary KidneyMihaela LitovcencoÎncă nu există evaluări
- Price List 2 Maret 2021Document10 paginiPrice List 2 Maret 2021Galih Wicaksono, MDÎncă nu există evaluări
- Listening Sample Test 3 Question PaperDocument5 paginiListening Sample Test 3 Question PaperjeznerÎncă nu există evaluări
- Dialysis in Malaysia: EditorialDocument3 paginiDialysis in Malaysia: EditorialfisplÎncă nu există evaluări
- Ketuban Pecah Dini Pada Kehamilan Prematur (KPD) / Preterm Premature Rupture of Membrane (Pprom), Last Update: 1 Februari 2017Document9 paginiKetuban Pecah Dini Pada Kehamilan Prematur (KPD) / Preterm Premature Rupture of Membrane (Pprom), Last Update: 1 Februari 2017Jonathan JonesÎncă nu există evaluări
- IDT - 8 v1 Waste ManagementDocument13 paginiIDT - 8 v1 Waste ManagementOzzyÎncă nu există evaluări
- Anti-Asthmatic Potential of Dried Draco SpilopterusDocument6 paginiAnti-Asthmatic Potential of Dried Draco SpilopterusNxxxÎncă nu există evaluări
- Ethanolic Extract of Doxorubicin On MCF-7 Breast Cancer CellDocument9 paginiEthanolic Extract of Doxorubicin On MCF-7 Breast Cancer Cellnugroho akhbarÎncă nu există evaluări
- Formularium 2014 - RS. Elisabeth PwkertoDocument53 paginiFormularium 2014 - RS. Elisabeth PwkertoayuÎncă nu există evaluări
- Methods of Speech Therapy Treatment For Stable Dysarthria A ReviewDocument14 paginiMethods of Speech Therapy Treatment For Stable Dysarthria A ReviewDavid Trujillo BEatoÎncă nu există evaluări
- Tooth DecayDocument28 paginiTooth DecayRyan Carlo CondeÎncă nu există evaluări
- Available To Relocate: Emmanuel Mamvura Mobile: +263777333072 & +263772557335: Location: Harare, Zimbabwe ProfileDocument2 paginiAvailable To Relocate: Emmanuel Mamvura Mobile: +263777333072 & +263772557335: Location: Harare, Zimbabwe ProfileHope CharakupaÎncă nu există evaluări
- Running Head: As Good As It Gets: An Analysis 1Document11 paginiRunning Head: As Good As It Gets: An Analysis 1Yassi FernandezÎncă nu există evaluări
- Ch03 Lecture Lifting and Moving PatientsDocument58 paginiCh03 Lecture Lifting and Moving Patientsnoer8180% (1)
- Introduction To Peritoneal Dialysis: Renal Self Learning PackageDocument12 paginiIntroduction To Peritoneal Dialysis: Renal Self Learning PackageArun PatilÎncă nu există evaluări