S-ar putea să vă placă și
- Food and Drug InteractionDocument2 paginiFood and Drug InteractionrxdocÎncă nu există evaluări
- Drugs To Watch With WARFARINDocument3 paginiDrugs To Watch With WARFARINRajendra RaiÎncă nu există evaluări
- Chapter 18 Common Drugs PDFDocument221 paginiChapter 18 Common Drugs PDFlalallalaÎncă nu există evaluări
- PharmecogenomicsDocument21 paginiPharmecogenomicsRatan Ratan100% (1)
- Drug Interactions: What Is An Interaction?Document4 paginiDrug Interactions: What Is An Interaction?Leyla MajundaÎncă nu există evaluări
- Routes of Drug Administration: Asst Professor Dept of Pharmacology Govt Medical College, AkolaDocument27 paginiRoutes of Drug Administration: Asst Professor Dept of Pharmacology Govt Medical College, Akolaنور الهدىÎncă nu există evaluări
- General Pharmacology - Sources of Drugs and Routes of AdministrationDocument48 paginiGeneral Pharmacology - Sources of Drugs and Routes of AdministrationDhriti Brahma78% (9)
- NSAIDs (Nonsteroidal Anti-Inflammatory Drugs): An OverviewDe la EverandNSAIDs (Nonsteroidal Anti-Inflammatory Drugs): An OverviewÎncă nu există evaluări
- Pharmacokinetics and Pharmacodynamics 40Document40 paginiPharmacokinetics and Pharmacodynamics 40Shoaib BiradarÎncă nu există evaluări
- Ranitidine Tramadol Ketorolac Ampicillin Paracetamol Drug StudyDocument10 paginiRanitidine Tramadol Ketorolac Ampicillin Paracetamol Drug Studyshiramu91% (11)
- Autacoids: Group No. 1Document92 paginiAutacoids: Group No. 1Rohan Pal100% (1)
- Antiviral Drugs Acting Against RNA Viruses: HIV: PHRM 412Document57 paginiAntiviral Drugs Acting Against RNA Viruses: HIV: PHRM 412Apurba Sarker ApuÎncă nu există evaluări
- Principles of Pharmacology Chapter 1Document37 paginiPrinciples of Pharmacology Chapter 1Muhammad ZakriaÎncă nu există evaluări
- Pharmacology: Nepthali Christuar Aldueza, R.N. Calamba Doctors CollegeDocument49 paginiPharmacology: Nepthali Christuar Aldueza, R.N. Calamba Doctors CollegeArielle Joy Atienza100% (1)
- Anti EmeticsDocument29 paginiAnti EmeticsBezawit TsigeÎncă nu există evaluări
- Fundamentals of PharmacyDocument66 paginiFundamentals of PharmacyLHYRA KATHLEEN LOPEZ100% (1)
- GastritisDocument6 paginiGastritisNader Smadi100% (5)
- 07 Dosage RegimenDocument44 pagini07 Dosage Regimenzetttttttttt100% (3)
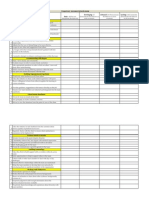
- Competency Assessment QuestionnaireDocument2 paginiCompetency Assessment QuestionnairekurutalaÎncă nu există evaluări
- PharmacologyDocument57 paginiPharmacologyarun231187Încă nu există evaluări
- Chrono Pharmaco LDocument46 paginiChrono Pharmaco LJaved AliÎncă nu există evaluări
- Rational Use of AntibioticsDocument32 paginiRational Use of AntibioticsRendy SusantoÎncă nu există evaluări
- Adrenergic and NonadrenergicDocument49 paginiAdrenergic and Nonadrenergicsweta sumanÎncă nu există evaluări
- Unit I General PharmacologyDocument16 paginiUnit I General PharmacologycuolyÎncă nu există evaluări
- EcosanoidsDocument21 paginiEcosanoidsfmduniaÎncă nu există evaluări
- Cholinergic and AnticholinergicDocument77 paginiCholinergic and Anticholinergicsweta sumanÎncă nu există evaluări
- Anti-Anginal and Antiischemic Drugs: Dr. Pradeepa H D Clinical PharmacologistDocument25 paginiAnti-Anginal and Antiischemic Drugs: Dr. Pradeepa H D Clinical PharmacologistpradeephdÎncă nu există evaluări
- PK-PD of Antimicrobial Therapy-Lecture12 Oct11Document37 paginiPK-PD of Antimicrobial Therapy-Lecture12 Oct11Idrissou FmsbÎncă nu există evaluări
- Drug Absorption and DistributionDocument30 paginiDrug Absorption and DistributionaelmowafyÎncă nu există evaluări
- DRUG Interactions of Veterinary ImportanceDocument8 paginiDRUG Interactions of Veterinary ImportanceSunil100% (1)
- Principles of PharmacotherapyDocument40 paginiPrinciples of Pharmacotherapyjunitria13Încă nu există evaluări
- Prescription CriticismDocument12 paginiPrescription CriticismRahul RavteÎncă nu există evaluări
- The Drug Act 1976Document24 paginiThe Drug Act 1976Wàrìs Ràfìqùé ßàlòçhÎncă nu există evaluări
- NORADRENALINE (Norepinephrine) : Presentation DescriptionDocument3 paginiNORADRENALINE (Norepinephrine) : Presentation DescriptionMutiaraÎncă nu există evaluări
- Adverse Drug ReactionsDocument21 paginiAdverse Drug Reactionspharma000100% (1)
- Ethiopia National Drug FormularyDocument572 paginiEthiopia National Drug FormularyportosinÎncă nu există evaluări
- Antibiotics: Presenter: Naila InamDocument41 paginiAntibiotics: Presenter: Naila InamInam KhanÎncă nu există evaluări
- Pharmacology Practical Manual - Student Copy2Document11 paginiPharmacology Practical Manual - Student Copy2NareshÎncă nu există evaluări
- Anti Ulcer DrugsDocument25 paginiAnti Ulcer DrugsPam LalaÎncă nu există evaluări
- Rational Use of Antibiotics STDocument32 paginiRational Use of Antibiotics STArita Rahmadarni100% (1)
- Practical 1-Far 161-FinishDocument10 paginiPractical 1-Far 161-FinishZulkifli Khairuddin100% (1)
- Argus 5 1 Test CasesDocument11 paginiArgus 5 1 Test CasespponnapatiÎncă nu există evaluări
- Introduction To PharmacologyDocument28 paginiIntroduction To Pharmacologynadar shahÎncă nu există evaluări
- Nanoparticles in Cancer Therapy and DiagnosisDocument55 paginiNanoparticles in Cancer Therapy and Diagnosismimshin0% (1)
- KAPS Pharmacist Syllabus The PharmapediaDocument3 paginiKAPS Pharmacist Syllabus The PharmapediaSanam ThahaÎncă nu există evaluări
- Gastrointestinal Tract Drugs: Pharmacist Marwan QasimDocument20 paginiGastrointestinal Tract Drugs: Pharmacist Marwan QasimWaliÎncă nu există evaluări
- Pharmacology of The GITDocument31 paginiPharmacology of The GITmarviecute22Încă nu există evaluări
- Antibiotics 9Document11 paginiAntibiotics 9Beth Morales100% (1)
- Opioid Analgesics: Just in Time Training September 2006Document16 paginiOpioid Analgesics: Just in Time Training September 2006Yel CMÎncă nu există evaluări
- Autocoids and Their AntagonistsDocument19 paginiAutocoids and Their AntagonistsHossein Sehati100% (1)
- 7 - Cholinomimetic DrugsDocument50 pagini7 - Cholinomimetic DrugslalitrajindoliaÎncă nu există evaluări
- Antithyroid Drugs by Sejal Khuman Advanced phARMACOLGY 2Document29 paginiAntithyroid Drugs by Sejal Khuman Advanced phARMACOLGY 2Sejal khumanÎncă nu există evaluări
- Sem 5/unit-3 Autocoids & Related DrugsDocument28 paginiSem 5/unit-3 Autocoids & Related DrugsDARSHAN BhirudÎncă nu există evaluări
- Anti-Rheumatoid Arthritis DrugsDocument57 paginiAnti-Rheumatoid Arthritis Drugsapi-306036754Încă nu există evaluări
- 47-Drug Acting On Skin and MucousDocument3 pagini47-Drug Acting On Skin and MucousMuhammad Sarmad MalikÎncă nu există evaluări
- AntibioticsDocument36 paginiAntibioticsBen Paolo Cecilia RabaraÎncă nu există evaluări
- AntiemeticsDocument25 paginiAntiemeticsPridho GaziansyahÎncă nu există evaluări
- 02.tablets (-II-)Document42 pagini02.tablets (-II-)Subha ShankareeÎncă nu există evaluări
- Posology 151223081101Document24 paginiPosology 151223081101eswarÎncă nu există evaluări
- Drug Induced Pulmonary DiseasesDocument26 paginiDrug Induced Pulmonary Diseaseswiona morasÎncă nu există evaluări
- Antiplatelet and Thrombolytic DrugsDocument48 paginiAntiplatelet and Thrombolytic DrugsNofa PuspitaÎncă nu există evaluări
- Pharmacotherapy For SchizophreniaDocument17 paginiPharmacotherapy For SchizophreniaNadya SaptarinaÎncă nu există evaluări
- Drug InteractionDocument2 paginiDrug InteractionNicole EncinaresÎncă nu există evaluări
- Drug Induced Hepatitis: Dr.M.Sharmila Assistant Professor M7 (Prof CR Unit) Institute of Internal MedicineDocument21 paginiDrug Induced Hepatitis: Dr.M.Sharmila Assistant Professor M7 (Prof CR Unit) Institute of Internal MedicineAtakan Yeşil100% (1)
- CBM Impact (April 2014) : Training Manager'S Name: Anil RamakrishnanDocument2 paginiCBM Impact (April 2014) : Training Manager'S Name: Anil RamakrishnankurutalaÎncă nu există evaluări
- Chatpata Orange SnackDocument2 paginiChatpata Orange SnackkurutalaÎncă nu există evaluări
- Names To Be Deleted From TracerDocument2 paginiNames To Be Deleted From TracerkurutalaÎncă nu există evaluări
- CBM Impact (April 2014) : Training Manager'S Name: Anil RamakrishnanDocument2 paginiCBM Impact (April 2014) : Training Manager'S Name: Anil RamakrishnankurutalaÎncă nu există evaluări
- Agenda Touch PPDocument19 paginiAgenda Touch PPkurutalaÎncă nu există evaluări
- Touch Untrained FsoDocument2 paginiTouch Untrained FsokurutalaÎncă nu există evaluări
- DRIVE PROGRAM (2013 - 2014) : Total Total Total TotalDocument1 paginăDRIVE PROGRAM (2013 - 2014) : Total Total Total TotalkurutalaÎncă nu există evaluări
- Glenmark HO Travel Details TemplateDocument4 paginiGlenmark HO Travel Details TemplatekurutalaÎncă nu există evaluări
- Dubagest SR Story Page 1Document1 paginăDubagest SR Story Page 1kurutalaÎncă nu există evaluări
- Milieus DetailingDocument2 paginiMilieus DetailingkurutalaÎncă nu există evaluări
- Esoz - Detailing TalkDocument2 paginiEsoz - Detailing TalkkurutalaÎncă nu există evaluări
- AnnouncementDocument1 paginăAnnouncementkurutalaÎncă nu există evaluări
- Program Name Division Name Date Duration of Days TimeDocument2 paginiProgram Name Division Name Date Duration of Days TimekurutalaÎncă nu există evaluări
- Milieus DetailingDocument2 paginiMilieus DetailingkurutalaÎncă nu există evaluări
- 11 Elovera Baby CreamDocument36 pagini11 Elovera Baby CreamkurutalaÎncă nu există evaluări
- TOUCH Untrained Status (January 2014)Document2 paginiTOUCH Untrained Status (January 2014)kurutalaÎncă nu există evaluări
- Vocarb DetailingDocument1 paginăVocarb DetailingkurutalaÎncă nu există evaluări
- Ascoril Expectorant - Detailing Story InterviewsDocument2 paginiAscoril Expectorant - Detailing Story InterviewskurutalaÎncă nu există evaluări
- SR No Division Brand: Division Wise Brands For Interview PanelDocument1 paginăSR No Division Brand: Division Wise Brands For Interview PanelkurutalaÎncă nu există evaluări
- La Shield DetailingDocument2 paginiLa Shield DetailingkurutalaÎncă nu există evaluări
- Healtheon DetailingDocument1 paginăHealtheon DetailingkurutalaÎncă nu există evaluări
- Hair4U VA CommunicationDocument4 paginiHair4U VA CommunicationkurutalaÎncă nu există evaluări
- Dubagest SR Story Page 1Document1 paginăDubagest SR Story Page 1kurutalaÎncă nu există evaluări
- Respiraory - VAF Detailing TalkDocument1 paginăRespiraory - VAF Detailing TalkkurutalaÎncă nu există evaluări
- Detailing Scalpe VafDocument3 paginiDetailing Scalpe VafkurutalaÎncă nu există evaluări
- Glenmark CV DetailingDocument1 paginăGlenmark CV DetailingkurutalaÎncă nu există evaluări
- Yearly Calender CDG ' 12-13 FinalDocument6 paginiYearly Calender CDG ' 12-13 FinalkurutalaÎncă nu există evaluări
- CTV DetailingDocument1 paginăCTV DetailingkurutalaÎncă nu există evaluări
- Critica VAF Detailing TalkDocument1 paginăCritica VAF Detailing TalkkurutalaÎncă nu există evaluări
- The Science Behind AspirinDocument14 paginiThe Science Behind AspirindipetÎncă nu există evaluări
- Updated 2022Document71 paginiUpdated 2022Nalimae Joseph CÎncă nu există evaluări
- Bioequivalence Study With Two Naproxen Sodium Tablet Formulations in Healthy Subjects Jbb.1000005Document11 paginiBioequivalence Study With Two Naproxen Sodium Tablet Formulations in Healthy Subjects Jbb.1000005tiaktuyonoÎncă nu există evaluări
- Analgetik Antipiretik AntiinflamasiDocument76 paginiAnalgetik Antipiretik AntiinflamasiranifebÎncă nu există evaluări
- BurnsDocument33 paginiBurnsErina Erichan Oto100% (1)
- Analgesicos No Opiodes No Esteroideos y Cox SelectivosDocument14 paginiAnalgesicos No Opiodes No Esteroideos y Cox SelectivosXY PragmaÎncă nu există evaluări
- Meloxicam 7.5 MG Daily and Naproxen 750Document7 paginiMeloxicam 7.5 MG Daily and Naproxen 750kwadwobrosÎncă nu există evaluări
- Ototoxic BrochureDocument6 paginiOtotoxic BrochureWindaÎncă nu există evaluări
- Ankle Sprain Medical BackgroundDocument13 paginiAnkle Sprain Medical BackgroundWilyam SerilÎncă nu există evaluări
- Lupus: PrintDocument24 paginiLupus: Printmelodia gandezaÎncă nu există evaluări
- OTC DrugsDocument29 paginiOTC DrugsHossam ArafaÎncă nu există evaluări
- AINS and EyeDocument26 paginiAINS and EyeEcaterina Borovic-PavlovschiÎncă nu există evaluări
- Nonsteroidal Antiinflammatorydrugsfor Acuteandchronicpain: Timothy J. Atkinson,, Jeffrey FudinDocument13 paginiNonsteroidal Antiinflammatorydrugsfor Acuteandchronicpain: Timothy J. Atkinson,, Jeffrey FudinMaBe MejíaÎncă nu există evaluări
- Diclofenac From Administration To Adverse Effect A Mini-ReviewDocument5 paginiDiclofenac From Administration To Adverse Effect A Mini-ReviewInternational Journal of Innovative Science and Research TechnologyÎncă nu există evaluări
- NCMB 316Document36 paginiNCMB 316Venansius GanggusÎncă nu există evaluări
- Over-The-Counter Medications in PregnancyDocument8 paginiOver-The-Counter Medications in PregnancyKenef CheungÎncă nu există evaluări
- Drugs Pregnancy CategoryDocument14 paginiDrugs Pregnancy CategoryDevi RachmawatiÎncă nu există evaluări
- Treatment of Ankylosing SpondylitisDocument16 paginiTreatment of Ankylosing SpondylitisrazvanbaranÎncă nu există evaluări
- Nursing Math Practice Questions, Answers, and TechniquesDocument118 paginiNursing Math Practice Questions, Answers, and Techniquesyaneidys perezÎncă nu există evaluări
- Pharmaceutical Side Effects Google SquareDocument267 paginiPharmaceutical Side Effects Google SquareCharlie HareÎncă nu există evaluări
- Analgesics in PeriodonticsDocument43 paginiAnalgesics in PeriodonticsRicha BhosaleÎncă nu există evaluări
- Diagnosisandtreatmentof Goutandpseudogoutfor EverydaypracticeDocument24 paginiDiagnosisandtreatmentof Goutandpseudogoutfor EverydaypracticePutri Aswariyah RamliÎncă nu există evaluări
- Bp503t Pcol Unit-IIIDocument38 paginiBp503t Pcol Unit-IIIAakkkÎncă nu există evaluări
- Degenerative Disc DiseaseDocument13 paginiDegenerative Disc Diseasehouki shanaÎncă nu există evaluări
- AntipyreticsDocument20 paginiAntipyreticsJoshua VillarbaÎncă nu există evaluări