S-ar putea să vă placă și
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Fractures: Dr. Pradeep Fernando MS, FRCSDocument31 paginiFractures: Dr. Pradeep Fernando MS, FRCSrikarzÎncă nu există evaluări
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Postintern15 07 2014letterDocument2 paginiPostintern15 07 2014letterrikarzÎncă nu există evaluări
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- ABC TraumaDocument27 paginiABC TraumarikarzÎncă nu există evaluări
- Fluid and Electrolyte TherapyDocument39 paginiFluid and Electrolyte TherapyrikarzÎncă nu există evaluări
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- An Approach To The Problem of Low Back PainDocument35 paginiAn Approach To The Problem of Low Back PainrikarzÎncă nu există evaluări
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Fluid and Electrolyte TherapyDocument39 paginiFluid and Electrolyte TherapyrikarzÎncă nu există evaluări
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- 04 Toxic GasesDocument30 pagini04 Toxic GasesrikarzÎncă nu există evaluări
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Batch 17 Tutorial 1Document5 paginiBatch 17 Tutorial 1rikarzÎncă nu există evaluări
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Thrombocytopenia: DR Chamilka JayasingheDocument31 paginiThrombocytopenia: DR Chamilka JayasingherikarzÎncă nu există evaluări
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Tute 13Document24 paginiTute 13rikarzÎncă nu există evaluări
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Acute Renal Failure: DR S. RatnayakeDocument19 paginiAcute Renal Failure: DR S. RatnayakerikarzÎncă nu există evaluări
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Tumour Immunology: Prof Anura WeerasingheDocument18 paginiTumour Immunology: Prof Anura WeerasingherikarzÎncă nu există evaluări
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- TuteDocument6 paginiTuterikarzÎncă nu există evaluări
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- Immunotherapy: Prof Anura WeerasingheDocument17 paginiImmunotherapy: Prof Anura WeerasingherikarzÎncă nu există evaluări
- 1 Mapsss000710 r1 Aqt90 Flex Brochure en LowDocument7 pagini1 Mapsss000710 r1 Aqt90 Flex Brochure en LowTW RHKLÎncă nu există evaluări
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
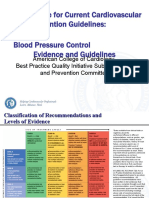
- 3 ACC Prevention Blood PressureDocument69 pagini3 ACC Prevention Blood PressureMelissa Delgado100% (1)
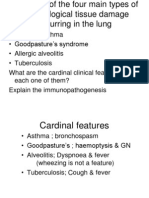
- Hypersensitivity ReactionsDocument12 paginiHypersensitivity ReactionsSphinxÎncă nu există evaluări
- LUMOS - DementiaDocument100 paginiLUMOS - DementiasamuelÎncă nu există evaluări
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- Learnin G Objectiv ESDocument54 paginiLearnin G Objectiv ESKirk Matthew ZhuÎncă nu există evaluări
- Cumulative Trauma DisordersDocument5 paginiCumulative Trauma Disordersravinaj21100% (1)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- Acupuncture and Cancer Pain: Yan Cui Magram and Gary E. DengDocument4 paginiAcupuncture and Cancer Pain: Yan Cui Magram and Gary E. DengirmaÎncă nu există evaluări
- Artikel Bahan Ujian PraktikumDocument10 paginiArtikel Bahan Ujian PraktikumTakiaGenjiÎncă nu există evaluări
- Hypertensive Crisis: - Alexter John C. Fajardo M.DDocument49 paginiHypertensive Crisis: - Alexter John C. Fajardo M.DAlexter John Cabalonga FajardoÎncă nu există evaluări
- Therapeutic Apheresis Operator Competency Aug06Document43 paginiTherapeutic Apheresis Operator Competency Aug06Jose Gregorio Riobueno BolivarÎncă nu există evaluări
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Parkinson's Disease Psychosis: Presentation, Diagnosis and ManagementDocument12 paginiParkinson's Disease Psychosis: Presentation, Diagnosis and ManagementEduardo Santana SuárezÎncă nu există evaluări
- Ebr - F&e OxygenationDocument1 paginăEbr - F&e OxygenationDARLENE ROSE BONGCAWILÎncă nu există evaluări
- A Psychosomatic Perspective On Endometriosis - A MDocument18 paginiA Psychosomatic Perspective On Endometriosis - A MsilsilviasilÎncă nu există evaluări
- Severe Ulcerative Colitis UHL Childrens Medical GuidelineDocument8 paginiSevere Ulcerative Colitis UHL Childrens Medical GuidelineFanny PritaningrumÎncă nu există evaluări
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Chapter 20 Prep U.odtDocument9 paginiChapter 20 Prep U.odtShade ElugbajuÎncă nu există evaluări
- CPG DyslipidemiaDocument26 paginiCPG DyslipidemiaRenzy SalumbreÎncă nu există evaluări
- Introduction & Epidemiology Clinical Features: End-Stage Renal Disease (ESRD)Document2 paginiIntroduction & Epidemiology Clinical Features: End-Stage Renal Disease (ESRD)Nikki VillanuevaÎncă nu există evaluări
- CH 084 Oral ThrushDocument7 paginiCH 084 Oral ThrushSavir GuptaÎncă nu există evaluări
- Basic First Aid NotesDocument9 paginiBasic First Aid NotesPaul SealyÎncă nu există evaluări
- Daftar Pustaka Semua 1-4Document8 paginiDaftar Pustaka Semua 1-4Yuni IsnayantiÎncă nu există evaluări
- Breast Abscess ManagementDocument10 paginiBreast Abscess Managementطلال العمريÎncă nu există evaluări
- OIIQ Prep QuestionsDocument10 paginiOIIQ Prep QuestionsDan Thanh Luu67% (3)
- Review: Arthritis in LeprosyDocument6 paginiReview: Arthritis in LeprosyadlestariÎncă nu există evaluări
- Peace Corps Vaccine Administration Schedule - TG 300 Medical Technical Guideline 300 - July 2008Document4 paginiPeace Corps Vaccine Administration Schedule - TG 300 Medical Technical Guideline 300 - July 2008Accessible Journal Media: Peace Corps Documents100% (1)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- New Inborn Error of MetabolismDocument45 paginiNew Inborn Error of Metabolismmannan mangal100% (1)
- Holoxan Pi PDFDocument18 paginiHoloxan Pi PDFKarol IonasÎncă nu există evaluări
- Laporan Jaga 5Document44 paginiLaporan Jaga 5Dila AuÎncă nu există evaluări
- ParkinsonDocument24 paginiParkinsonSandy AgustianÎncă nu există evaluări
- Benefits of Blood DonationDocument1 paginăBenefits of Blood DonationljxÎncă nu există evaluări
- Oceanic Question Bank Year 4Document358 paginiOceanic Question Bank Year 4maryÎncă nu există evaluări
- The Game: Penetrating the Secret Society of Pickup ArtistsDe la EverandThe Game: Penetrating the Secret Society of Pickup ArtistsEvaluare: 4 din 5 stele4/5 (131)