S-ar putea să vă placă și
- Geriatric Soap NoteDocument6 paginiGeriatric Soap Noteapi-282282363100% (6)
- Kerry Layne Author Albert Ferro Author 100 Cases in Clinical PharmacologyDocument249 paginiKerry Layne Author Albert Ferro Author 100 Cases in Clinical Pharmacologyteju100% (3)
- Trusted Medical Answers-In Seconds.: Lipid DisordersDocument13 paginiTrusted Medical Answers-In Seconds.: Lipid DisordersMohammed shamiul Shahid100% (1)
- Inflammatory Bowel DiseaseDocument14 paginiInflammatory Bowel Diseasehazelel100% (1)
- Basic Computations 2 IV & IVFDocument37 paginiBasic Computations 2 IV & IVFCarl Elexer Cuyugan Ano100% (5)
- Managing The Bladder and Bowel in Spina BifidaDocument77 paginiManaging The Bladder and Bowel in Spina BifidaSeptinaAyuSamsiati100% (1)
- Medics PHC Protocols 3rd EditionDocument102 paginiMedics PHC Protocols 3rd EditionLee HillÎncă nu există evaluări
- Raynaud's Disease - JERAIZADocument23 paginiRaynaud's Disease - JERAIZAmaU439Încă nu există evaluări
- Iritable Bowel SyndromeDocument30 paginiIritable Bowel SyndromeArnella HutagalungÎncă nu există evaluări
- CholilithiasisDocument94 paginiCholilithiasisdr.hendraÎncă nu există evaluări
- Inflammatory Bowel DiseaseDocument42 paginiInflammatory Bowel DiseaseCarmelli Mariae Calugay100% (2)
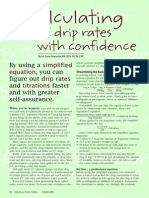
- Streamline I.V. drip calculations with simplified equationsDocument4 paginiStreamline I.V. drip calculations with simplified equationsmydewyboyÎncă nu există evaluări
- Shock and BleedingDocument24 paginiShock and BleedingRaissa IcaÎncă nu există evaluări
- Ear Disorder Multiple Choice Questions-RationaleDocument5 paginiEar Disorder Multiple Choice Questions-Rationalemydewyboy83% (6)
- PATHOMA Fundamentals of Pathology 2018 PDFDocument232 paginiPATHOMA Fundamentals of Pathology 2018 PDFRafael Eduardo Toro Manotas100% (2)
- Inflammatory Bowel Diseases: Dr. Evelyn Angie M. BiomedDocument36 paginiInflammatory Bowel Diseases: Dr. Evelyn Angie M. BiomedAnnisÎncă nu există evaluări
- River BlindnessDocument5 paginiRiver BlindnessBello SakanauÎncă nu există evaluări
- Clinical Features of Renal DiseaseDocument80 paginiClinical Features of Renal DiseaseIdiAmadouÎncă nu există evaluări
- Gastritis: Medical AffairDocument11 paginiGastritis: Medical AffairKomal KhanÎncă nu există evaluări
- Peptic UlcerDocument31 paginiPeptic UlcerHarpal Bajwa0% (1)
- Renal Calculi: Urolithiasis, Nephrolithiasis, Renal StoneDocument18 paginiRenal Calculi: Urolithiasis, Nephrolithiasis, Renal StonerohitÎncă nu există evaluări
- IBDDocument27 paginiIBDKatarina SilalahiÎncă nu există evaluări
- Peptic Ulcer DiseaseDocument36 paginiPeptic Ulcer DiseaseRamanujam SekarÎncă nu există evaluări
- Entry To Practice CompetenciesDocument20 paginiEntry To Practice CompetenciesmydewyboyÎncă nu există evaluări
- ####Bahan Kuliah ISK Blok 23 (Nov 2015)Document32 pagini####Bahan Kuliah ISK Blok 23 (Nov 2015)ajengdmrÎncă nu există evaluări
- Bacterial Urinary Tract Infections (UTIs): Causes, Symptoms and TreatmentDocument27 paginiBacterial Urinary Tract Infections (UTIs): Causes, Symptoms and TreatmentNaseem Bin Yoosaf100% (1)
- Hirschprung DiseaseDocument9 paginiHirschprung DiseaseRajeev JhaÎncă nu există evaluări
- Hepatitis BDocument12 paginiHepatitis BTeti AndriÎncă nu există evaluări
- Triage in The HospitalDocument15 paginiTriage in The HospitalCarie Manarondong100% (1)
- GI Tract Food Pathway GuideDocument22 paginiGI Tract Food Pathway GuideElpen FatrizalÎncă nu există evaluări
- Nu'man AS DaudDocument23 paginiNu'man AS DaudHidayat BazeherÎncă nu există evaluări
- Sample QuestionnaireDocument10 paginiSample QuestionnaireJess Fernandez BorgaÎncă nu există evaluări
- URINARY TRACT INFECTION CAUSES AND TREATMENTDocument6 paginiURINARY TRACT INFECTION CAUSES AND TREATMENTLourdes Fernandez CabreraÎncă nu există evaluări
- Intestinal Obstruction: EpidemiologyDocument11 paginiIntestinal Obstruction: EpidemiologyBereket temesgenÎncă nu există evaluări
- Urinary Stones DiseaseDocument40 paginiUrinary Stones DiseaseRenaldy ThiorisÎncă nu există evaluări
- Pathognomonic Signs of DiseasesDocument4 paginiPathognomonic Signs of DiseasesmydewyboyÎncă nu există evaluări
- Communicable Diseases Nursing Study BulletsDocument2 paginiCommunicable Diseases Nursing Study Bulletsɹǝʍdןnos100% (9)
- Communicable Diseases Nursing Study BulletsDocument2 paginiCommunicable Diseases Nursing Study Bulletsɹǝʍdןnos100% (9)
- Communicable Diseases Nursing Study BulletsDocument2 paginiCommunicable Diseases Nursing Study Bulletsɹǝʍdןnos100% (9)
- Inflammatory Bowel DiseasesDocument30 paginiInflammatory Bowel DiseasesMohammedHuzairIbunuAbidÎncă nu există evaluări
- Management of Inflammatory Bowel Disease: Dr. Sumithra AppavaDocument43 paginiManagement of Inflammatory Bowel Disease: Dr. Sumithra AppavadrcumeeÎncă nu există evaluări
- Ulcerative Colitis: DR Syed Ubaid Associate Professor of SurgeryDocument71 paginiUlcerative Colitis: DR Syed Ubaid Associate Professor of SurgeryFachry Al RafiqiÎncă nu există evaluări
- Powerpoint: Chronic Inflammatory DisordesDocument55 paginiPowerpoint: Chronic Inflammatory Disordesj.doe.hex_87Încă nu există evaluări
- Inflammatory Bowel DiseaseDocument12 paginiInflammatory Bowel DiseasemoonsoundÎncă nu există evaluări
- Bacterial MeningitisDocument43 paginiBacterial MeningitisAthit Wutthisanwatthana100% (1)
- Abdominal Wall Extraskeletal Ewing Sarcoma - Case ReportDocument3 paginiAbdominal Wall Extraskeletal Ewing Sarcoma - Case ReportInternational Organization of Scientific Research (IOSR)Încă nu există evaluări
- Brucellosis 2Document70 paginiBrucellosis 2Zara IftikharÎncă nu există evaluări
- Salivary Gland DisordersDocument30 paginiSalivary Gland DisordersSangeeta BSRÎncă nu există evaluări
- Ewing SarcomaDocument4 paginiEwing SarcomaNurulAqilahZulkifliÎncă nu există evaluări
- Reproductive Tract InfectionDocument48 paginiReproductive Tract InfectionSampriti Roy100% (1)
- Pathophysiology of InfectionDocument3 paginiPathophysiology of Infectionchristianemmanuel18Încă nu există evaluări
- Tetanus RabiesDocument67 paginiTetanus RabiesWaNda GrÎncă nu există evaluări
- Intestinal ObstructionDocument6 paginiIntestinal ObstructionCling Cruza0% (1)
- Tetanus: Causes, Symptoms, Treatment and PreventionDocument102 paginiTetanus: Causes, Symptoms, Treatment and PreventionMo Oo MooÎncă nu există evaluări
- What is Lichen Planus and Lichenoid MucositisDocument7 paginiWhat is Lichen Planus and Lichenoid MucositisNurul AfiahÎncă nu există evaluări
- Gastric and Duodenal UlcerDocument19 paginiGastric and Duodenal UlcerEnerolisa ParedesÎncă nu există evaluări
- Infectious and Inflammatory Disorders of The Urinary SystemDocument16 paginiInfectious and Inflammatory Disorders of The Urinary SystemBibi Renu100% (1)
- WILMs TumorDocument3 paginiWILMs TumorLorie May GuillangÎncă nu există evaluări
- Perichondritis PinnaDocument2 paginiPerichondritis PinnaAnish RajÎncă nu există evaluări
- Chole CystDocument12 paginiChole CystMoch NizamÎncă nu există evaluări
- Burkitt Lymphoma: Teacher: Daniel Hernández. Student: Diana Rosales DominguezDocument16 paginiBurkitt Lymphoma: Teacher: Daniel Hernández. Student: Diana Rosales DominguezDianita Rosales Dominguez100% (1)
- Intestinal Atresia and StenosisDocument7 paginiIntestinal Atresia and StenosisMichael NafarinÎncă nu există evaluări
- Intraventricular Hemorrhage (IVH) : Intensive Care Nursery House Staff ManualDocument3 paginiIntraventricular Hemorrhage (IVH) : Intensive Care Nursery House Staff Manualjimzz44Încă nu există evaluări
- Case Control DesignDocument42 paginiCase Control DesignHope EkwensiÎncă nu există evaluări
- EENT Disorders StudentsDocument26 paginiEENT Disorders StudentsPye Antwan DelvaÎncă nu există evaluări
- ANDI Classification System Explains Benign Breast DisordersDocument9 paginiANDI Classification System Explains Benign Breast DisordersaprooolÎncă nu există evaluări
- Anal Fissure Guide: Causes, Symptoms and TreatmentsDocument14 paginiAnal Fissure Guide: Causes, Symptoms and TreatmentsAnonymous LoQcj2xEÎncă nu există evaluări
- Diverticular DiseaseDocument15 paginiDiverticular DiseaseRogie SaludoÎncă nu există evaluări
- Heart & Hemodynamics NotesDocument8 paginiHeart & Hemodynamics NotesBrandice BradleyÎncă nu există evaluări
- Diabetes MellitusDocument17 paginiDiabetes MellitusRuqayya KobatteÎncă nu există evaluări
- HIV Natural History StagesDocument10 paginiHIV Natural History StagesNirav Sharma100% (1)
- Paget Disease of Bone, A Simple Guide to the Condition, Treatment and Related DiseasesDe la EverandPaget Disease of Bone, A Simple Guide to the Condition, Treatment and Related DiseasesÎncă nu există evaluări
- Gastric Outlet Obstruction, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDe la EverandGastric Outlet Obstruction, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsÎncă nu există evaluări
- Inflammatory Bowel Disease IBDDocument24 paginiInflammatory Bowel Disease IBDKhadeer AGÎncă nu există evaluări
- Drug Study - M.nancy 20414Document7 paginiDrug Study - M.nancy 20414mydewyboyÎncă nu există evaluări
- Cord Care Methods: Chlorhexidine Best for Detachment and Infection PreventionDocument2 paginiCord Care Methods: Chlorhexidine Best for Detachment and Infection PreventionmydewyboyÎncă nu există evaluări
- Lap Cholecystectomy Better Than OCDocument7 paginiLap Cholecystectomy Better Than OCmydewyboyÎncă nu există evaluări
- IV Fluid CommonDocument1 paginăIV Fluid CommonmydewyboyÎncă nu există evaluări
- Basic Computations 2 IV IVFDocument37 paginiBasic Computations 2 IV IVFmydewyboyÎncă nu există evaluări
- JurnalDocument12 paginiJurnalIrara RaÎncă nu există evaluări
- Emergency DrugsDocument17 paginiEmergency DrugsmydewyboyÎncă nu există evaluări
- Avoid Meds ErrorDocument15 paginiAvoid Meds ErrormydewyboyÎncă nu există evaluări
- Medication CalculationsDocument5 paginiMedication Calculationsmydewyboy100% (1)
- OB Emergency ArticleDocument11 paginiOB Emergency ArticlemydewyboyÎncă nu există evaluări
- DRUGS PoisoningDocument76 paginiDRUGS PoisoningmydewyboyÎncă nu există evaluări
- Lumbar & Sacral VertebraeDocument1 paginăLumbar & Sacral VertebraemydewyboyÎncă nu există evaluări
- Triage PowerpointDocument28 paginiTriage PowerpointmydewyboyÎncă nu există evaluări
- Therapeutic Touch Help Reduce Pain in Cancer Pt-ResearchDocument9 paginiTherapeutic Touch Help Reduce Pain in Cancer Pt-ResearchmydewyboyÎncă nu există evaluări
- PQRSTDocument64 paginiPQRSTiduhilagÎncă nu există evaluări
- Daniel Ryan TsutsuDocument1 paginăDaniel Ryan TsutsumydewyboyÎncă nu există evaluări
- Explore the world of nursing in the ORDocument2 paginiExplore the world of nursing in the ORmydewyboyÎncă nu există evaluări
- Explore the world of nursing in the ORDocument2 paginiExplore the world of nursing in the ORmydewyboyÎncă nu există evaluări
- Therapeutic Touch Help Reduce Pain in Cancer Pt-ResearchDocument9 paginiTherapeutic Touch Help Reduce Pain in Cancer Pt-ResearchmydewyboyÎncă nu există evaluări
- American Cancer Society 2013 TrendsDocument44 paginiAmerican Cancer Society 2013 TrendsPearl DiBerardinoÎncă nu există evaluări
- Ersoy-Pruritus 5 D Itch ScaleDocument7 paginiErsoy-Pruritus 5 D Itch ScaleyosefÎncă nu există evaluări
- Rds NRP 2021Document33 paginiRds NRP 2021Aiwi Goddard MurilloÎncă nu există evaluări
- Laporan Kasus BronkopneumoniaDocument30 paginiLaporan Kasus BronkopneumoniaShifa Ali JannatinÎncă nu există evaluări
- Gov. Abbott OpenTexas ReportDocument64 paginiGov. Abbott OpenTexas ReportAnonymous Pb39klJ92% (12)
- HCC (Kuliah DR Masrul)Document38 paginiHCC (Kuliah DR Masrul)Tengku M Ridho AnharÎncă nu există evaluări
- CERT+Basic Unit+4+Participant+Manual EnglishDocument19 paginiCERT+Basic Unit+4+Participant+Manual EnglishBrandon OlsenÎncă nu există evaluări
- ECSI Instructor Update 2021Document52 paginiECSI Instructor Update 2021Zach MatthewsÎncă nu există evaluări
- Barrier MethodDocument3 paginiBarrier MethodJaninaPatriciaBÎncă nu există evaluări
- Web KFOG-jan-11Document16 paginiWeb KFOG-jan-11kutra3000Încă nu există evaluări
- The Cotton DriverDocument2 paginiThe Cotton DriverDanny Eduardo RomeroÎncă nu există evaluări
- Data Obat Lengkap-SIAP IMPORTDocument9 paginiData Obat Lengkap-SIAP IMPORTRegita Ragil SejahteraÎncă nu există evaluări
- My-MRCP-notes-st1 and 3 by Dr-NadimDocument93 paginiMy-MRCP-notes-st1 and 3 by Dr-NadimSaidunnessa IrinÎncă nu există evaluări
- Covid 19 y Vacuna PfizerDocument13 paginiCovid 19 y Vacuna PfizerSMIBA MedicinaÎncă nu există evaluări
- Heart Structure and FunctionsDocument3 paginiHeart Structure and FunctionsChristella KateÎncă nu există evaluări
- Tests From The Database Croc 2Document30 paginiTests From The Database Croc 2Андрій ВознякÎncă nu există evaluări
- Managing Chronic Kidney Disease: Treatment Options and ComplicationsDocument4 paginiManaging Chronic Kidney Disease: Treatment Options and ComplicationsSheena CabrilesÎncă nu există evaluări
- Overview of TonsillectomyDocument8 paginiOverview of TonsillectomyMaya PutriÎncă nu există evaluări
- Faculty of Medicine and Health Sciences Score Sheet For CASE Write-UpDocument30 paginiFaculty of Medicine and Health Sciences Score Sheet For CASE Write-UpJared Khoo Er HauÎncă nu există evaluări
- Detrusor InstabilityDocument7 paginiDetrusor Instabilityapi-3705046Încă nu există evaluări
- Case Sheet for Maternity ServicesDocument22 paginiCase Sheet for Maternity ServicesGulfeshan ArshiÎncă nu există evaluări
- D5imb IvDocument1 paginăD5imb IvSeno HyeonÎncă nu există evaluări
- Paracetamol Overdose: BW 40 KG Without Fluid RestrictionDocument2 paginiParacetamol Overdose: BW 40 KG Without Fluid RestrictionAndy TanÎncă nu există evaluări
- OMR SPOTTERS With AnswersDocument15 paginiOMR SPOTTERS With Answersblessy winsletÎncă nu există evaluări
- Schreibman - Radiology of Joint Disease - My Practical ApproachDocument16 paginiSchreibman - Radiology of Joint Disease - My Practical ApproachborstÎncă nu există evaluări
- Case History Sample AnalyzedDocument6 paginiCase History Sample AnalyzedeinsteinÎncă nu există evaluări