S-ar putea să vă placă și
- TWIS, Fluid and Electrolytes-4Document45 paginiTWIS, Fluid and Electrolytes-4Madison FÎncă nu există evaluări
- Acute Diabetic Ketoacidosis (DKA)Document21 paginiAcute Diabetic Ketoacidosis (DKA)Madhu Sudhan Pandeya0% (1)
- Somchodok Chakreeyarat, MD. Endocrine Unit, Department of Medicine Bhumibol Adulyadej HospitalDocument53 paginiSomchodok Chakreeyarat, MD. Endocrine Unit, Department of Medicine Bhumibol Adulyadej HospitalLing TaerahkunÎncă nu există evaluări
- Electrolyte ImbalanceDocument44 paginiElectrolyte ImbalanceDevi Christina Damanik (Papua medical School)Încă nu există evaluări
- Ketoasidosis DiabetikDocument18 paginiKetoasidosis DiabetikDanti PutriÎncă nu există evaluări
- DR Omar Kamal Ansari Dept of AnaesthesiologyDocument46 paginiDR Omar Kamal Ansari Dept of Anaesthesiologyvvb_frndÎncă nu există evaluări
- Diabetic EmergencyDocument28 paginiDiabetic Emergencychandrima pattadarÎncă nu există evaluări
- Diabetic Ketoacidosis (DKA) - Presentation Slide EditedDocument22 paginiDiabetic Ketoacidosis (DKA) - Presentation Slide EditedTerence Chin0% (1)
- Diabetic KetoacidosisDocument27 paginiDiabetic Ketoacidosisjun sianÎncă nu există evaluări
- Diabetic Ketoacidosis in PaediatricDocument11 paginiDiabetic Ketoacidosis in PaediatricSana Anam JahanÎncă nu există evaluări
- Review: Diagnostic and Treatment of Electrolyte DisturbancesDocument31 paginiReview: Diagnostic and Treatment of Electrolyte DisturbancesalvyandaniÎncă nu există evaluări
- Red Eye by DR MainuddinDocument38 paginiRed Eye by DR MainuddinMainuddin HasanÎncă nu există evaluări
- DKAPPTxDocument34 paginiDKAPPTxMuhammad FurqanÎncă nu există evaluări
- Cme Fluid and Electrolytes 2902016Document37 paginiCme Fluid and Electrolytes 2902016Mohd Faie Ramli0% (1)
- Sagraves MSfluids Lytes 2004Document59 paginiSagraves MSfluids Lytes 2004Burhan Ul HaqÎncă nu există evaluări
- Diabetic Ketoacidosis (DKA) : Prepared By:yazan Masaied Instructor:Abed AsakrahDocument15 paginiDiabetic Ketoacidosis (DKA) : Prepared By:yazan Masaied Instructor:Abed Asakrahzyazan329Încă nu există evaluări
- Pass Critical Care Endocrine Frcem ResourcesDocument41 paginiPass Critical Care Endocrine Frcem ResourcesYoussef SaadÎncă nu există evaluări
- DkaDocument36 paginiDkaSumit KhetarpalÎncă nu există evaluări
- HypocalcemiaDocument34 paginiHypocalcemiaClaudia IrimieÎncă nu există evaluări
- Diabetic Emergencies by DR Gireesh Kumar K P, Department of Emergency Medicine, Amrita Institute of Medical Sciences, KochiDocument23 paginiDiabetic Emergencies by DR Gireesh Kumar K P, Department of Emergency Medicine, Amrita Institute of Medical Sciences, KochiSreekrishnan Trikkur100% (2)
- 1 - Fluid and Electrolytes (Schwartz Based)Document52 pagini1 - Fluid and Electrolytes (Schwartz Based)Alexandra RebosuraÎncă nu există evaluări
- Fluid and ElectrolyteDocument71 paginiFluid and ElectrolytePratishtha SinghÎncă nu există evaluări
- Diabetc Keto AcidosisDocument13 paginiDiabetc Keto AcidosisVijiÎncă nu există evaluări
- Hyperglycemic Crisis in Acute Care: Purwoko Sugeng HDocument49 paginiHyperglycemic Crisis in Acute Care: Purwoko Sugeng HBee DanielÎncă nu există evaluări
- Keseimbangan Elektrolit Dan Asam Basa: Dr. Satriawan Abadi, SP - Pd-KicDocument79 paginiKeseimbangan Elektrolit Dan Asam Basa: Dr. Satriawan Abadi, SP - Pd-KicInterna FKUNHASÎncă nu există evaluări
- DKA Concepts and ManagementDocument22 paginiDKA Concepts and ManagementMohammad AliÎncă nu există evaluări
- Acute Renal FailureDocument5 paginiAcute Renal FailureSalman KhanÎncă nu există evaluări
- Hippo EM Board Review - Electrolyte Emergencies Written SummaryDocument5 paginiHippo EM Board Review - Electrolyte Emergencies Written SummaryMichael IvanÎncă nu există evaluări
- Endocrine Emergencies CompiledDocument102 paginiEndocrine Emergencies CompiledSubhkanish RavindraÎncă nu există evaluări
- Diabetic EmergenciesDocument65 paginiDiabetic EmergenciesManmeet SÎncă nu există evaluări
- New Format MasterDocument34 paginiNew Format MasterMuhammad FurqanÎncă nu există evaluări
- Terapi CairanDocument30 paginiTerapi CairanNunik Dewi KumalasariÎncă nu există evaluări
- Fluids & Electrolytes: Scott G. Sagraves, MD, FACSDocument59 paginiFluids & Electrolytes: Scott G. Sagraves, MD, FACSAsad Khan KhalilÎncă nu există evaluări
- Dr. Mohamed Ali Hamedh - DKA - 2023Document25 paginiDr. Mohamed Ali Hamedh - DKA - 2023ÁýáFáŕőúgÎncă nu există evaluări
- DKA For PEMDocument26 paginiDKA For PEMTemesgen AyanaÎncă nu există evaluări
- Management of Potassium Disorders 17706 ArticleDocument4 paginiManagement of Potassium Disorders 17706 ArticlealeÎncă nu există evaluări
- Diabetes Emergencies ComplicationsDocument30 paginiDiabetes Emergencies Complicationsosamafoud7710Încă nu există evaluări
- Hypokalemia: Jazeel Owayed Rata'anDocument9 paginiHypokalemia: Jazeel Owayed Rata'anraed faisalÎncă nu există evaluări
- EMERGENCIES IN DM (KAD Dan HHS)Document26 paginiEMERGENCIES IN DM (KAD Dan HHS)ozÎncă nu există evaluări
- Principle of Fluid & Electrolyte Management in ADocument47 paginiPrinciple of Fluid & Electrolyte Management in AAbdulazeez Abdulmalik100% (1)
- Common Electrolyte Disturbances and Management Edited 2023Document46 paginiCommon Electrolyte Disturbances and Management Edited 2023abdurabengÎncă nu există evaluări
- Final Common Medical Surgical EmergenciesDocument99 paginiFinal Common Medical Surgical Emergenciesapi-195799092Încă nu există evaluări
- Fluids and Electrolytes For Pediatrics: Natharina YolandaDocument45 paginiFluids and Electrolytes For Pediatrics: Natharina YolandaTe HineahuoneÎncă nu există evaluări
- 2.2 Fluid & ElectrolytesDocument80 pagini2.2 Fluid & ElectrolytesAizza ZarateÎncă nu există evaluări
- Keseimbangan Elektrolit Dan Asam Basa: Dr. Satriawan Abadi, SP - Pd-KicDocument79 paginiKeseimbangan Elektrolit Dan Asam Basa: Dr. Satriawan Abadi, SP - Pd-KicSteven KatuukÎncă nu există evaluări
- Endocrine EmergenciesDocument52 paginiEndocrine EmergenciesAdi ParamarthaÎncă nu există evaluări
- DKA FinalDocument66 paginiDKA FinalllaychinÎncă nu există evaluări
- CP2 A Mnemonic For The TreatDocument15 paginiCP2 A Mnemonic For The Treateng78ineÎncă nu există evaluări
- DIURETICSDocument39 paginiDIURETICSFrancisÎncă nu există evaluări
- Dka and HHSDocument25 paginiDka and HHSMouhammad Dawoud100% (2)
- Acute Effects of Diabetes MellitusDocument17 paginiAcute Effects of Diabetes MellitussaminingÎncă nu există evaluări
- Fluid and Electrolyte Therapy - SeblewongelDocument47 paginiFluid and Electrolyte Therapy - SeblewongelSeblewongel AsemeÎncă nu există evaluări
- Dka 1Document45 paginiDka 1jomanabuhaniyehÎncă nu există evaluări
- Diabetic KetoacidosisDocument38 paginiDiabetic KetoacidosisAwatef AbushhiwaÎncă nu există evaluări
- Electrolyte ImbalanceDocument44 paginiElectrolyte ImbalanceTiven StiveÎncă nu există evaluări
- Diabetic KetoacidosisDocument39 paginiDiabetic KetoacidosisNathasya B.W.Încă nu există evaluări
- Renal Emergency RevisiDocument103 paginiRenal Emergency Revisidesy f sarahÎncă nu există evaluări
- Case Study: Diabetic KetoacidosisDocument66 paginiCase Study: Diabetic Ketoacidosisllaychin100% (2)
- Diabetic Ketoacidosis Acute Management: A State of Absolute Insulin BankruptcyDocument24 paginiDiabetic Ketoacidosis Acute Management: A State of Absolute Insulin BankruptcyGwEn LimÎncă nu există evaluări
- Isnacc Membership Form 2019Document2 paginiIsnacc Membership Form 2019Anto PaulÎncă nu există evaluări
- Admission To Post Graduate Medical Degree/Diploma Courses - 2015 Option ListDocument2 paginiAdmission To Post Graduate Medical Degree/Diploma Courses - 2015 Option ListAnto PaulÎncă nu există evaluări
- Pgm2017 ProsDocument76 paginiPgm2017 ProsAnto PaulÎncă nu există evaluări
- CPD Jaundice PDFDocument53 paginiCPD Jaundice PDFAnto PaulÎncă nu există evaluări
- NME CY Approvals (12 31 2010)Document2 paginiNME CY Approvals (12 31 2010)Anto PaulÎncă nu există evaluări
- Tyvak PlatformsDocument1 paginăTyvak PlatformsNguyenÎncă nu există evaluări
- 9701 w19 QP 21 PDFDocument12 pagini9701 w19 QP 21 PDFFaiza KhalidÎncă nu există evaluări
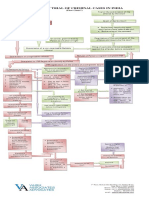
- Process of Trial of Criminal Cases in India (Flow Chart)Document1 paginăProcess of Trial of Criminal Cases in India (Flow Chart)Arun Hiro100% (1)
- PWC Taxavvy 18 2020 Mco PDFDocument12 paginiPWC Taxavvy 18 2020 Mco PDFMichael YapÎncă nu există evaluări
- Easy Trade Manager Forex RobotDocument10 paginiEasy Trade Manager Forex RobotPinda DhanoyaÎncă nu există evaluări
- Italian Companies Eastern China - JAN 2014Document139 paginiItalian Companies Eastern China - JAN 2014AndresÎncă nu există evaluări
- Tribebook Wendigo Revised Edition 6244638Document109 paginiTribebook Wendigo Revised Edition 6244638PedroÎncă nu există evaluări
- Reflections: The Sol JournalDocument13 paginiReflections: The Sol Journalapi-268650070Încă nu există evaluări
- Influence of Brand Experience On CustomerDocument16 paginiInfluence of Brand Experience On Customerarif adrianÎncă nu există evaluări
- MCQ Class VDocument9 paginiMCQ Class VSneh MahajanÎncă nu există evaluări
- Financial Fitness ChecklistDocument4 paginiFinancial Fitness Checklistcoach_22Încă nu există evaluări
- Walsh January Arrest Sherrif Records Pgs 10601-10700Document99 paginiWalsh January Arrest Sherrif Records Pgs 10601-10700columbinefamilyrequest100% (1)
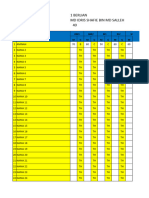
- TEMPLATE Keputusan Peperiksaan THP 1Document49 paginiTEMPLATE Keputusan Peperiksaan THP 1SABERI BIN BANDU KPM-GuruÎncă nu există evaluări
- Everyday Use AnalysisDocument8 paginiEveryday Use AnalysisThe 3d PlanetÎncă nu există evaluări
- Jee Mathmatic PaperDocument16 paginiJee Mathmatic PaperDeepesh KumarÎncă nu există evaluări
- Stock Market Prediction Using Machine Learning ProposalDocument10 paginiStock Market Prediction Using Machine Learning ProposalBilal AhmedÎncă nu există evaluări
- ECAT STD 2 Sample Question PaperDocument7 paginiECAT STD 2 Sample Question PaperVinay Jindal0% (1)
- National Highways Authority of IndiaDocument3 paginiNational Highways Authority of IndiaRohitÎncă nu există evaluări
- PRE-TEST (World Religion)Document3 paginiPRE-TEST (World Religion)Marc Sealtiel ZunigaÎncă nu există evaluări
- Huawei Videoconferencing MCU VP9600 Series Data SheetDocument2 paginiHuawei Videoconferencing MCU VP9600 Series Data SheetIsaac PiresÎncă nu există evaluări
- Security Operating Procedures and StandardsDocument5 paginiSecurity Operating Procedures and StandardsQuy Tranxuan100% (2)
- Pineapple Working PaperDocument57 paginiPineapple Working PaperAnonymous EAineTiz100% (7)
- 3 - Accounting For Loans and ImpairmentDocument1 pagină3 - Accounting For Loans and ImpairmentReese AyessaÎncă nu există evaluări
- TV Studio ChainDocument38 paginiTV Studio ChainKalpesh Katara100% (1)
- 2019 - List of Equipment, Tools & MaterialsDocument3 pagini2019 - List of Equipment, Tools & Materialsreynald manzanoÎncă nu există evaluări
- Assignment 1684490923Document16 paginiAssignment 1684490923neha.engg45755Încă nu există evaluări
- MahoyoDocument6 paginiMahoyoChriz HunterÎncă nu există evaluări
- (I) (Ii) (Iii) (Iv) : Nahata Professional Academy Q1. Choose The Correct AnswerDocument5 pagini(I) (Ii) (Iii) (Iv) : Nahata Professional Academy Q1. Choose The Correct AnswerBurhanuddin BohraÎncă nu există evaluări
- 659.69 BM67 2018-02-06 02 Im Beu-UsaDocument88 pagini659.69 BM67 2018-02-06 02 Im Beu-UsaIrakli JibladzeÎncă nu există evaluări
- Effects of Changes in Foreign Exchange Rates Ias 21Document11 paginiEffects of Changes in Foreign Exchange Rates Ias 21cykenÎncă nu există evaluări