S-ar putea să vă placă și
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Congenital Glaucomas: 1. Primary 2. Iridocorneal DysgenesisDocument12 paginiCongenital Glaucomas: 1. Primary 2. Iridocorneal DysgenesiskhadzxÎncă nu există evaluări
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (587)
- Dermatologic DiseasesDocument2 paginiDermatologic DiseaseskhadzxÎncă nu există evaluări
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (890)
- 34 Idiopathic Spec Uveitis SyndromeDocument8 pagini34 Idiopathic Spec Uveitis SyndromekhadzxÎncă nu există evaluări
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- 6th Central Pay Commission Salary CalculatorDocument15 pagini6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- Metabolic Bone DiseaseDocument29 paginiMetabolic Bone DiseasekhadzxÎncă nu există evaluări
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- 13 Peripheral Corneal InflamDocument5 pagini13 Peripheral Corneal InflamkhadzxÎncă nu există evaluări
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Acquired 2. Isolated Familial Ectopia Lentis 3. Associated With Systemic SyndromesDocument8 paginiAcquired 2. Isolated Familial Ectopia Lentis 3. Associated With Systemic SyndromeskhadzxÎncă nu există evaluări
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Primary Angle-Closure Glaucoma: 1. Pathogenesis 2. ClassificationDocument9 paginiPrimary Angle-Closure Glaucoma: 1. Pathogenesis 2. ClassificationkhadzxÎncă nu există evaluări
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- 28primary Open Angle GlaucomaDocument21 pagini28primary Open Angle GlaucomakhadzxÎncă nu există evaluări
- 12conjunctival TumoursDocument12 pagini12conjunctival TumourskhadzxÎncă nu există evaluări
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Congenital Cataract: 1. Important FactsDocument13 paginiCongenital Cataract: 1. Important FactskhadzxÎncă nu există evaluări
- Juvenile Rheumatoid Arthritis (Jra) (Juvenile Chronic Arthritis-Jca)Document70 paginiJuvenile Rheumatoid Arthritis (Jra) (Juvenile Chronic Arthritis-Jca)khadzxÎncă nu există evaluări
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Abnormal Lens ShapeDocument4 paginiAbnormal Lens ShapekhadzxÎncă nu există evaluări
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- 15corneal InfectionsDocument8 pagini15corneal InfectionskhadzxÎncă nu există evaluări
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2219)
- 09conjunctival InfectionsDocument11 pagini09conjunctival InfectionskhadzxÎncă nu există evaluări
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- 02chronic Marginal BlepharitisDocument7 pagini02chronic Marginal BlepharitiskhadzxÎncă nu există evaluări
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Ndiang'Ui: Unexpected Deaths 24 September 2009Document25 paginiNdiang'Ui: Unexpected Deaths 24 September 2009khadzxÎncă nu există evaluări
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (265)
- Disorders of Eye LashesDocument8 paginiDisorders of Eye LasheskhadzxÎncă nu există evaluări
- Poisoning by MedicinesDocument11 paginiPoisoning by MedicineskhadzxÎncă nu există evaluări
- Postmortem Changes and Postmortem Time IntervalDocument24 paginiPostmortem Changes and Postmortem Time IntervalkhadzxÎncă nu există evaluări
- Chronic Osteomyelitis in Early Infancy: Presenter: DR Maina Discussant: DR Mogire (Orthopedic Surgeon)Document27 paginiChronic Osteomyelitis in Early Infancy: Presenter: DR Maina Discussant: DR Mogire (Orthopedic Surgeon)khadzxÎncă nu există evaluări
- External Fixation of The Lower Limb 2Document13 paginiExternal Fixation of The Lower Limb 2khadzxÎncă nu există evaluări
- Sudden Unexpected Death FMT 400Document11 paginiSudden Unexpected Death FMT 400khadzxÎncă nu există evaluări
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Narcotics N HallucinogensDocument14 paginiNarcotics N HallucinogenskhadzxÎncă nu există evaluări
- Introduction To Forensic Medicine DR David Chumba MBCHB, Mmed (Human Pathology), Dip. For Med (Sa)Document20 paginiIntroduction To Forensic Medicine DR David Chumba MBCHB, Mmed (Human Pathology), Dip. For Med (Sa)khadzxÎncă nu există evaluări
- Introduction To Forensic Medicine DR David Chumba MBCHB, Mmed (Human Pathology), Dip. For Med (Sa)Document20 paginiIntroduction To Forensic Medicine DR David Chumba MBCHB, Mmed (Human Pathology), Dip. For Med (Sa)khadzxÎncă nu există evaluări
- Fire Arm Injuries 4th Yr ForensicDocument31 paginiFire Arm Injuries 4th Yr ForensickhadzxÎncă nu există evaluări
- Carbon Monoxide Poisoning 4th YrDocument17 paginiCarbon Monoxide Poisoning 4th YrkhadzxÎncă nu există evaluări
- Classification of Injuries FMTDocument30 paginiClassification of Injuries FMTkhadzx100% (2)
- Malocclusion and Orthodontic Eldoret 2009Document33 paginiMalocclusion and Orthodontic Eldoret 2009khadzxÎncă nu există evaluări
- Basic Life Support (BLS) in Adults - UpToDateDocument11 paginiBasic Life Support (BLS) in Adults - UpToDateAFA.BLSÎncă nu există evaluări
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (119)
- Dr. Madaan Anatomy MCQ 2-2 (Muhadharaty)Document46 paginiDr. Madaan Anatomy MCQ 2-2 (Muhadharaty)Joseph Brima SambaÎncă nu există evaluări
- Non-Steroidal Anti-Inflammatory Drugs (Nsaids) : Dr. Nishant B. BhansaliDocument24 paginiNon-Steroidal Anti-Inflammatory Drugs (Nsaids) : Dr. Nishant B. Bhansaliankit ahirÎncă nu există evaluări
- Med Surg 1Document33 paginiMed Surg 1SSA CommissionÎncă nu există evaluări
- Nur 111 Session 7 Sas 1Document8 paginiNur 111 Session 7 Sas 1Zzimply Tri Sha UmaliÎncă nu există evaluări
- 1.1. Pocus en Emg y Critical Care 2018 PDFDocument8 pagini1.1. Pocus en Emg y Critical Care 2018 PDFEmergencias RebagliatiÎncă nu există evaluări
- The Pathophysiology of Elevated Vitamin B12 in Clinical PracticeDocument11 paginiThe Pathophysiology of Elevated Vitamin B12 in Clinical PracticePanagiotis-Sokratis LoumakisÎncă nu există evaluări
- Fry Et Al 2017Document9 paginiFry Et Al 2017Ernest YipÎncă nu există evaluări
- Chest Pain Case PresentationDocument24 paginiChest Pain Case PresentationAnonymous 17awurSUÎncă nu există evaluări
- Hematology Oncology - Anemia ApproachDocument1 paginăHematology Oncology - Anemia ApproachEugen MÎncă nu există evaluări
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- RHEUMATOID ARTHYRITIS CASEDocument32 paginiRHEUMATOID ARTHYRITIS CASEJune Faith HacheroÎncă nu există evaluări
- Cardiovascular Physiology Case 9Document50 paginiCardiovascular Physiology Case 9Kim AcostaÎncă nu există evaluări
- CLINICAL CHEMISTRY GUIDEDocument10 paginiCLINICAL CHEMISTRY GUIDEDeniel BusiÎncă nu există evaluări
- The Final FRCR Self-AssessmentDocument244 paginiThe Final FRCR Self-AssessmentAman KumarÎncă nu există evaluări
- Haematological Parameters and Lipid Profile AbnormDocument10 paginiHaematological Parameters and Lipid Profile AbnormPhelix O DaniyanÎncă nu există evaluări
- In2Med HaematologyDocument30 paginiIn2Med Haematologye148659Încă nu există evaluări
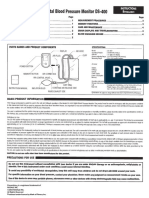
- Digital Blood Pressure Monitor DS-400: Parts Names and Product ComponentsDocument4 paginiDigital Blood Pressure Monitor DS-400: Parts Names and Product ComponentsJorÎncă nu există evaluări
- Powell 2022 Oi 221002 1664506604.73378Document12 paginiPowell 2022 Oi 221002 1664506604.73378AntoineÎncă nu există evaluări
- Vascular Disorder: DR Nur Asyilla Che Jalil Pathology Department PPSP HusmDocument140 paginiVascular Disorder: DR Nur Asyilla Che Jalil Pathology Department PPSP HusmHaziq KamardinÎncă nu există evaluări
- The Little Black Book of Ecg Secrets PDFDocument12 paginiThe Little Black Book of Ecg Secrets PDFamaandreiÎncă nu există evaluări
- Epithelial and connective tissue types in the human bodyDocument4 paginiEpithelial and connective tissue types in the human bodyrenee belle isturisÎncă nu există evaluări
- KDIGO 2023 CKD Guideline Public Review Draft 5 July 2023Document339 paginiKDIGO 2023 CKD Guideline Public Review Draft 5 July 2023oscar coreaÎncă nu există evaluări
- 26 (Ni Komang Sindy Octaviana Dewi 193213030)Document10 pagini26 (Ni Komang Sindy Octaviana Dewi 193213030)Sindy OctaÎncă nu există evaluări
- Istan Respiratory Deleted Learner)Document2 paginiIstan Respiratory Deleted Learner)Brandie StrangeÎncă nu există evaluări
- Statins Side Effects - Pain, Inflammation, and MoreDocument6 paginiStatins Side Effects - Pain, Inflammation, and MoreJeff TeeÎncă nu există evaluări
- 10 Early Signs of LupusDocument3 pagini10 Early Signs of LupusJessica RomeroÎncă nu există evaluări
- Medical Surgical Nursing 64 PagsDocument64 paginiMedical Surgical Nursing 64 Pagstanya nÎncă nu există evaluări
- Creatinine ClearanceDocument6 paginiCreatinine ClearancedianaÎncă nu există evaluări
- ProteinuriaDocument1 paginăProteinuriamutiara nurzaniÎncă nu există evaluări
- Drug Classification Indication Action and Pharmacokinetics Contraindication Adverse Effect Monitoring ParameterDocument5 paginiDrug Classification Indication Action and Pharmacokinetics Contraindication Adverse Effect Monitoring ParameteryssatÎncă nu există evaluări