S-ar putea să vă placă și
- Kidney NewDocument4 paginiKidney NewParth BhayanaÎncă nu există evaluări
- Gyneacology Revision by All TeamDocument14 paginiGyneacology Revision by All TeamSara EhabÎncă nu există evaluări
- NSAID's "Non-Steroidal Anti-Inflammatory Drugs": Mmbakhaitan@uqu - Edu.saDocument19 paginiNSAID's "Non-Steroidal Anti-Inflammatory Drugs": Mmbakhaitan@uqu - Edu.saAhmed HossamÎncă nu există evaluări
- Salmonela Thyposa: Disease Etiology Unique S&S Brief Patophysiology Diagnostic Treatment / Plan OthersDocument8 paginiSalmonela Thyposa: Disease Etiology Unique S&S Brief Patophysiology Diagnostic Treatment / Plan OthersNatalia_WiryantoÎncă nu există evaluări
- Diseases Link To Chromosomal Abnormalities: Chromoso Me Abnormality DiseaseDocument7 paginiDiseases Link To Chromosomal Abnormalities: Chromoso Me Abnormality Diseasenreena aslamÎncă nu există evaluări
- Gene Related DiseaseDocument3 paginiGene Related Diseasevivek govardhanamÎncă nu există evaluări
- Genitourinary System: Renal FailureDocument6 paginiGenitourinary System: Renal FailureEn ConejosÎncă nu există evaluări
- Present at 4-12 Months, Development Arrest From Pre-B To BDocument2 paginiPresent at 4-12 Months, Development Arrest From Pre-B To BWaoÎncă nu există evaluări
- Tumor Immunology: I. Common Tumor MarkersDocument2 paginiTumor Immunology: I. Common Tumor MarkersDivineGloryMalbuyoÎncă nu există evaluări
- A Bunch of Pharm ShitDocument2 paginiA Bunch of Pharm ShitkatÎncă nu există evaluări
- The Better You Get at Something, The More Enjoyable It Can BecomeDocument6 paginiThe Better You Get at Something, The More Enjoyable It Can BecomeAshÎncă nu există evaluări
- Differential Diagnosis of Genital Ulcer Differential Diagnosis of Genital UlcersDocument3 paginiDifferential Diagnosis of Genital Ulcer Differential Diagnosis of Genital UlcersNurhayati HasanahÎncă nu există evaluări
- Handouts Integumentary Sys Sp11 B201Document7 paginiHandouts Integumentary Sys Sp11 B201Kelly TrainorÎncă nu există evaluări
- Important Terms - Tropical InfectionDocument8 paginiImportant Terms - Tropical InfectionTimothy JordanÎncă nu există evaluări
- Bacterial Infections of The SkinDocument9 paginiBacterial Infections of The Skinbeia21Încă nu există evaluări
- CVR PharmacologyDocument6 paginiCVR PharmacologyRebecca MarshallÎncă nu există evaluări
- Abnormal LFTsDocument2 paginiAbnormal LFTsRenu RosyÎncă nu există evaluări
- Microbiology Summary DocumentDocument7 paginiMicrobiology Summary DocumentKÎncă nu există evaluări
- Nephrotic Syndrome WikipediaDocument10 paginiNephrotic Syndrome WikipediaJohn KevlarÎncă nu există evaluări
- Essential Update: FDA Approves First Test To Predict AKI in Critically Ill PatientsDocument5 paginiEssential Update: FDA Approves First Test To Predict AKI in Critically Ill PatientsRika Ariyanti SaputriÎncă nu există evaluări
- SYPHYLISDocument1 paginăSYPHYLISkhadzxÎncă nu există evaluări
- 'Aliah's Cardiovascular SystemDocument45 pagini'Aliah's Cardiovascular SystemLuqman Al-Bashir FauziÎncă nu există evaluări
- LeukemiaDocument2 paginiLeukemiaAyeshaArifÎncă nu există evaluări
- Renal SyndromeDocument13 paginiRenal SyndromeAndreas KristianÎncă nu există evaluări
- Virlogy Made AwesomeDocument6 paginiVirlogy Made AwesomeUsman Ali AkbarÎncă nu există evaluări
- Review For The 2° Semester Exam Alessandro Mo6a, UVVG, 3 YearDocument9 paginiReview For The 2° Semester Exam Alessandro Mo6a, UVVG, 3 Yeardjxela89Încă nu există evaluări
- Abdominal Wall, Omentum, Mesentery, RetroperitoneumDocument6 paginiAbdominal Wall, Omentum, Mesentery, RetroperitoneumMon Ordona De GuzmanÎncă nu există evaluări
- Semester 2 Drug ListDocument7 paginiSemester 2 Drug ListNam_Pham_6481Încă nu există evaluări
- Patho CA - Acute PancreatitisDocument1 paginăPatho CA - Acute PancreatitisKÎncă nu există evaluări
- Antimycobacterial Drugs PDFDocument3 paginiAntimycobacterial Drugs PDFCas BuÎncă nu există evaluări
- Staph. Aureus Staph. Epidermidis Staph. SaprophyticusDocument5 paginiStaph. Aureus Staph. Epidermidis Staph. SaprophyticusTom PedersonÎncă nu există evaluări
- Commensal AmoebaDocument2 paginiCommensal AmoebaCoy NuñezÎncă nu există evaluări
- DermDocument10 paginiDermyassrmarwaÎncă nu există evaluări
- Chronic Inflammatory Dermatoses Inflammatory Blistering DisordersDocument4 paginiChronic Inflammatory Dermatoses Inflammatory Blistering DisordersspringdingÎncă nu există evaluări
- Organism Description Drug of ChoiceDocument14 paginiOrganism Description Drug of ChoiceMary YongcoÎncă nu există evaluări
- The Immune System OhtDocument6 paginiThe Immune System OhtKa-Shun Leung100% (1)
- Goljan Live Notes Day 1Document5 paginiGoljan Live Notes Day 1Daniyal AzmatÎncă nu există evaluări
- CHEM-Year 2 Chemistry Cheat Sheet For EDEXCELDocument12 paginiCHEM-Year 2 Chemistry Cheat Sheet For EDEXCELraiabhijith586Încă nu există evaluări
- Antivirals, Rubella, Peecorna VIRUSDocument3 paginiAntivirals, Rubella, Peecorna VIRUSErnie G. Bautista II, RN, MDÎncă nu există evaluări
- Pelvis and Perineum Clinical CorrelationDocument4 paginiPelvis and Perineum Clinical CorrelationKeesha Mariel AlimonÎncă nu există evaluări
- PleuraDocument6 paginiPleuraameerabest100% (1)
- Histo Review 2Document13 paginiHisto Review 2Coy NuñezÎncă nu există evaluări
- Histology Viscus Flow ChartDocument1 paginăHistology Viscus Flow ChartNaser Hamdi ZalloumÎncă nu există evaluări
- Ultimate Pharm GuideDocument41 paginiUltimate Pharm GuideeanguyenÎncă nu există evaluări
- Viruses (B) PDFDocument4 paginiViruses (B) PDFLyka MahrÎncă nu există evaluări
- Study Product 1Document117 paginiStudy Product 1javibruinÎncă nu există evaluări
- Poliomyelitis Haemophilus Influenzae Type B VariecellaDocument4 paginiPoliomyelitis Haemophilus Influenzae Type B VariecellaJeanna Chong100% (1)
- Nephrotic Nephritic SyndromsDocument4 paginiNephrotic Nephritic SyndromsKimiwari100% (2)
- Anatomy and Physiology MnemonicsDocument7 paginiAnatomy and Physiology MnemonicsLalajimÎncă nu există evaluări
- WWW Cram Com Flashcards Hematology Slides 872178Document8 paginiWWW Cram Com Flashcards Hematology Slides 872178Anonymous t5TDwdÎncă nu există evaluări
- Complement SystemDocument4 paginiComplement SystemFait HeeÎncă nu există evaluări
- General Features of The Immune SystemDocument6 paginiGeneral Features of The Immune SystemMinerva Bautista RoseteÎncă nu există evaluări
- Cardio Block 3Document62 paginiCardio Block 3Maya LaPradeÎncă nu există evaluări
- Handouts Immune Defenses F11Document12 paginiHandouts Immune Defenses F11Kelly Trainor100% (1)
- 5 Cyto AbnormalDocument9 pagini5 Cyto AbnormalMerli Ann Joyce CalditoÎncă nu există evaluări
- Mean Standard Deviation: Antonio Mirano - 2018Document8 paginiMean Standard Deviation: Antonio Mirano - 2018jÎncă nu există evaluări
- Haemopoiesis: Composition of Whole Blood & Its ComponentsDocument8 paginiHaemopoiesis: Composition of Whole Blood & Its ComponentsSafiya JamesÎncă nu există evaluări
- Bam Slam Drug CardDocument4 paginiBam Slam Drug CardLeticia GonzalezÎncă nu există evaluări
- Anthropology: Anthropology Is The Scientific Study of Humans, Human BehaviorDocument26 paginiAnthropology: Anthropology Is The Scientific Study of Humans, Human BehaviorAliaÎncă nu există evaluări
- Pathology of Common Glomerular Syndromes: DR Purushotham KrishnappaDocument34 paginiPathology of Common Glomerular Syndromes: DR Purushotham KrishnappaTarin IslamÎncă nu există evaluări
- Henoch Schönlein PurpuraDocument14 paginiHenoch Schönlein PurpurasangheetaÎncă nu există evaluări
- Approach To Pale ChildDocument37 paginiApproach To Pale ChildsangheetaÎncă nu există evaluări
- NephroticDocument8 paginiNephroticsangheetaÎncă nu există evaluări
- Nephritic SyndromeDocument19 paginiNephritic SyndromesangheetaÎncă nu există evaluări
- Nephrotic SyndromeDocument40 paginiNephrotic SyndromesangheetaÎncă nu există evaluări
- Henoch Schönlein PurpuraDocument14 paginiHenoch Schönlein PurpurasangheetaÎncă nu există evaluări
- Industrial Training Final Report - 090308Document5 paginiIndustrial Training Final Report - 090308sangheetaÎncă nu există evaluări
- CPG Management of Cancer PainDocument90 paginiCPG Management of Cancer PainsangheetaÎncă nu există evaluări
- Cardiovascular ExaminationDocument3 paginiCardiovascular ExaminationsangheetaÎncă nu există evaluări
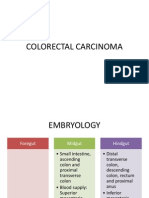
- Colorectal CarcinomaDocument117 paginiColorectal Carcinomasangheeta100% (1)
- Arthritis of Ankle and FootDocument28 paginiArthritis of Ankle and FootsangheetaÎncă nu există evaluări
- Post Traumatic Stress DisorderDocument14 paginiPost Traumatic Stress DisordersangheetaÎncă nu există evaluări
- Management of Diabetes FootDocument41 paginiManagement of Diabetes FootsangheetaÎncă nu există evaluări
- Management of Cervical CancerDocument29 paginiManagement of Cervical CancersangheetaÎncă nu există evaluări
- NSPNCDDocument41 paginiNSPNCDsangheetaÎncă nu există evaluări
- Management of Acute DiarrheaDocument2 paginiManagement of Acute DiarrheasangheetaÎncă nu există evaluări
- Benefits of Breast Feeding To MotherDocument7 paginiBenefits of Breast Feeding To MothersangheetaÎncă nu există evaluări
- Benefits of Breast Feeding To MotherDocument7 paginiBenefits of Breast Feeding To MothersangheetaÎncă nu există evaluări
- 007geneexpres recomDNA Obj&figDocument12 pagini007geneexpres recomDNA Obj&figsangheeta100% (2)
- TCA 88 Operating InstructionsDocument276 paginiTCA 88 Operating InstructionsRonald Sol Salen Jordas80% (5)
- Feasibility Study - Spa ResortDocument110 paginiFeasibility Study - Spa ResortMenchie Ella Diezmos Guno100% (2)
- 04 - QA Calibration Job Method For Packing Machine Check Weight 1Document3 pagini04 - QA Calibration Job Method For Packing Machine Check Weight 1Mohd A IshakÎncă nu există evaluări
- Annotated BibliographyDocument3 paginiAnnotated BibliographyJose FranciscoÎncă nu există evaluări
- Ineffective Health MaintenanceDocument1 paginăIneffective Health Maintenancedragon3466Încă nu există evaluări
- Admission MDS First CounsellingDocument3 paginiAdmission MDS First CounsellingavninderÎncă nu există evaluări
- Soal Tes 1 Sem 6 S1 Reg 2021Document3 paginiSoal Tes 1 Sem 6 S1 Reg 2021arka jrÎncă nu există evaluări
- Programme Guide Certificate in Community Health (BPCCHN) - CompressedDocument120 paginiProgramme Guide Certificate in Community Health (BPCCHN) - CompressedChakrapani ChaturvediÎncă nu există evaluări
- A Study To Assess The Knowledge of The Utility of Toilets and Hazards of Open Air Defecation Practice Among Rural Adults of Muchakandi VillageDocument6 paginiA Study To Assess The Knowledge of The Utility of Toilets and Hazards of Open Air Defecation Practice Among Rural Adults of Muchakandi VillageInternational Journal of Innovative Science and Research TechnologyÎncă nu există evaluări
- Marjan - Reflection About Mental HealthDocument1 paginăMarjan - Reflection About Mental HealthRhonna Aromin NavarroÎncă nu există evaluări
- Tendinopathy CourseDocument3 paginiTendinopathy CourseGoranMarkovicÎncă nu există evaluări
- Motivation PDFDocument1 paginăMotivation PDFAnonymous tBxCPAEX7SÎncă nu există evaluări
- NCPDocument11 paginiNCPJohnhineÎncă nu există evaluări
- Cartilage and OsteoarthritisDocument374 paginiCartilage and OsteoarthritisItai IzhakÎncă nu există evaluări
- Power Plate Group Ex Power Basic 1 PDFDocument4 paginiPower Plate Group Ex Power Basic 1 PDFRicardo OliveiraÎncă nu există evaluări
- Shell Gadus S3 Wirerope T: Performance, Features & Benefits Main ApplicationsDocument2 paginiShell Gadus S3 Wirerope T: Performance, Features & Benefits Main ApplicationssfkcrcnÎncă nu există evaluări
- CH 04 The Skeletal System (New)Document85 paginiCH 04 The Skeletal System (New)alyssa bananÎncă nu există evaluări
- Thesis Protocol Final SarangDocument26 paginiThesis Protocol Final SarangRaj KotichaÎncă nu există evaluări
- Rational-Emotive Behaviour Therapy (Rebt)Document11 paginiRational-Emotive Behaviour Therapy (Rebt)Sheralena Mohd RasidÎncă nu există evaluări
- Mind, Society and Behavior - World BankDocument236 paginiMind, Society and Behavior - World BankAnt Green100% (1)
- Pathophys BURNDocument2 paginiPathophys BURNpaupaulala83% (6)
- Translation and Validation of The Amsterdam Preoperative Anxiety and Information Scale (Apais) Into Hausa LanguageDocument23 paginiTranslation and Validation of The Amsterdam Preoperative Anxiety and Information Scale (Apais) Into Hausa LanguageGlobal Research and Development ServicesÎncă nu există evaluări
- Very Important Paper AyurvedaDocument4 paginiVery Important Paper Ayurvedaarun.sunaniya8701Încă nu există evaluări
- Bookshelf NBK401552Document24 paginiBookshelf NBK401552Hanina mamiÎncă nu există evaluări
- Past ContinuousDocument2 paginiPast ContinuousJoaquin GabilondoÎncă nu există evaluări
- Quality Assurance 608Document42 paginiQuality Assurance 608ENTREPRENEUR 8211Încă nu există evaluări
- A-Plus Early Criticalcare Brochure Full 20130529 FinalDocument18 paginiA-Plus Early Criticalcare Brochure Full 20130529 Finalnusthe2745Încă nu există evaluări
- Themythofmultitasking Rosen PDFDocument6 paginiThemythofmultitasking Rosen PDFyeni marcela montañaÎncă nu există evaluări
- Language Development: - Iphy OkoyeDocument9 paginiLanguage Development: - Iphy OkoyeIPHY OKOYEÎncă nu există evaluări
- NCERT Class 9 Political Science Chapter 6 YouTube Lecture HandoutsDocument5 paginiNCERT Class 9 Political Science Chapter 6 YouTube Lecture Handoutsarjun anjana anjanaÎncă nu există evaluări