S-ar putea să vă placă și
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (120)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Filetype PDF Complement PathwaysDocument2 paginiFiletype PDF Complement PathwaysScottÎncă nu există evaluări
- Arcanis Children of The Sky The Kio SourcebookDocument68 paginiArcanis Children of The Sky The Kio SourcebookMatthew AperÎncă nu există evaluări
- Mennyi Ideig Kell Vért Szívnia Egy Vámpírnak?Document2 paginiMennyi Ideig Kell Vért Szívnia Egy Vámpírnak?Vincze Miklós / 24.huÎncă nu există evaluări
- Latihan Soal Bahasa Inggris Sma Kelas X Semester 2Document14 paginiLatihan Soal Bahasa Inggris Sma Kelas X Semester 2tyasajeng100% (2)
- Animal Diversity 7th Edition Hickman Test Bank 1Document9 paginiAnimal Diversity 7th Edition Hickman Test Bank 1gregoryÎncă nu există evaluări
- Pre Columbian Art Including Selection of LempertzDocument148 paginiPre Columbian Art Including Selection of LempertzAQQUIROGA50% (2)
- Bangladesh: NiversityDocument50 paginiBangladesh: Niversitylokesh kumarÎncă nu există evaluări
- Sample Proposal For GrantDocument8 paginiSample Proposal For GrantRomee SinghÎncă nu există evaluări
- Basic Anatomy and Physiology of Brain and Spinal CordDocument59 paginiBasic Anatomy and Physiology of Brain and Spinal CorddrmalikarifÎncă nu există evaluări
- Bull Terrier Kills ChildDocument1 paginăBull Terrier Kills ChildsallyfrankenwarteÎncă nu există evaluări
- Subcutaneous Infections and True PathogensDocument2 paginiSubcutaneous Infections and True PathogensthescarletpimpernelsÎncă nu există evaluări
- Zak's Class SystemDocument115 paginiZak's Class SystemGeorge Quail100% (2)
- Psychophysiological Detection of Deception Analysis Ii - Course #503Document67 paginiPsychophysiological Detection of Deception Analysis Ii - Course #503John PrasetioÎncă nu există evaluări
- TaxonomiDocument22 paginiTaxonomiDiaz Busthomi FaiziÎncă nu există evaluări
- NCP Impaired Gas ExchangeDocument2 paginiNCP Impaired Gas ExchangeGabriel Tolentino70% (10)
- Harcourt GK Phonics Practice Book StudentDocument144 paginiHarcourt GK Phonics Practice Book StudentІрина КрупаÎncă nu există evaluări
- Chapter 18. LaryngoscopesDocument133 paginiChapter 18. Laryngoscopesadham08Încă nu există evaluări
- IFRS Case Studies Handout PDFDocument66 paginiIFRS Case Studies Handout PDFPrince RyanÎncă nu există evaluări
- Immunoglobulin A (Iga)Document1 paginăImmunoglobulin A (Iga)Lione MilanÎncă nu există evaluări
- Surviving Sepsis Hour 1 Bundle InfographDocument1 paginăSurviving Sepsis Hour 1 Bundle InfographLaura PutriÎncă nu există evaluări
- FSIS Product CategorizationDocument12 paginiFSIS Product Categorizationimran24Încă nu există evaluări
- Anterior Anatomy and The Science of A Natural Smile (OCR)Document146 paginiAnterior Anatomy and The Science of A Natural Smile (OCR)Alfonso Jimenez90% (10)
- Gender in English and ArabicDocument20 paginiGender in English and ArabicKhawla Adnan100% (1)
- Water Vascular System of StarfishDocument4 paginiWater Vascular System of StarfishCyanDesÎncă nu există evaluări
- WWW Healingqigong Org 8 Section BrocadeDocument8 paginiWWW Healingqigong Org 8 Section BrocadeqpidoneuroÎncă nu există evaluări
- Grade5 Unit1Document5 paginiGrade5 Unit1api-239494748Încă nu există evaluări
- The Mystery of Metamorphosis - Foreword by Lynn Margulis and Dorion SaganDocument5 paginiThe Mystery of Metamorphosis - Foreword by Lynn Margulis and Dorion SaganChelsea Green Publishing100% (1)
- Practice Subject and Verb IdentificationDocument4 paginiPractice Subject and Verb IdentificationAyuseptiÎncă nu există evaluări
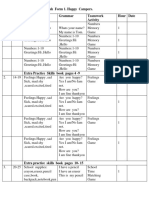
- English Form 1. Happy Campers. Unit Pages Vocabulary Grammar Teamwork Activity Hour DateDocument4 paginiEnglish Form 1. Happy Campers. Unit Pages Vocabulary Grammar Teamwork Activity Hour Dateİlkanə CabbarovaÎncă nu există evaluări
- 10 Myth About Tannin in SorghumDocument3 pagini10 Myth About Tannin in SorghumWilly YanuwarÎncă nu există evaluări