S-ar putea să vă placă și
- MANUAL CoachingSkills1 AS Nov2018Document39 paginiMANUAL CoachingSkills1 AS Nov2018irstarworkÎncă nu există evaluări
- Unit 3 - Roles of Professional Helper July 2016Document64 paginiUnit 3 - Roles of Professional Helper July 2016shirleechenchichiunÎncă nu există evaluări
- 3 Determinants of LearningDocument6 pagini3 Determinants of LearningKenÎncă nu există evaluări
- Community Needs Assessment Postpartum DepressionDocument26 paginiCommunity Needs Assessment Postpartum Depressionapi-607536364Încă nu există evaluări
- Induction, Deployment, Retaining, PromotionDocument40 paginiInduction, Deployment, Retaining, PromotionAyang TayengÎncă nu există evaluări
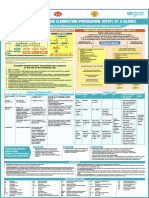
- NTEP at A Glance - Comprehensive Clinical Management Protocol For TBDocument1 paginăNTEP at A Glance - Comprehensive Clinical Management Protocol For TBNael NajeebÎncă nu există evaluări
- Decision MakingDocument20 paginiDecision MakingAshutosh SinghÎncă nu există evaluări
- Research Methodology: InterpretationDocument13 paginiResearch Methodology: Interpretationahsan habibÎncă nu există evaluări
- Delegation SanuDocument14 paginiDelegation SanuSANU RAMASWAMYÎncă nu există evaluări
- Fourteen Principles of Administration by Henri FayolDocument2 paginiFourteen Principles of Administration by Henri FayolanushavergheseÎncă nu există evaluări
- Implementing Plan of Action For Community HealthDocument58 paginiImplementing Plan of Action For Community HealthArthur Melbert Gallano100% (1)
- Chapter 6 Patients Subordinate Workplace and Professional AdvocacyDocument26 paginiChapter 6 Patients Subordinate Workplace and Professional AdvocacyCharles Avevrahamme M. AmlogÎncă nu există evaluări
- Format - Health Teaching PlanDocument5 paginiFormat - Health Teaching PlanRichie VilaÎncă nu există evaluări
- Presented By: Tamboli Amit S. First Year MSC (Psychiatric) Nursing Mimh PuneDocument25 paginiPresented By: Tamboli Amit S. First Year MSC (Psychiatric) Nursing Mimh PuneAmit Tamboli100% (1)
- Chapter 5 - Group DynamicsDocument7 paginiChapter 5 - Group DynamicsLord GrimÎncă nu există evaluări
- Course Plan On Nursing ManagementDocument8 paginiCourse Plan On Nursing ManagementshailaÎncă nu există evaluări
- Brief COPE Coping Strategies of Nurses QuestionnaireDocument5 paginiBrief COPE Coping Strategies of Nurses Questionnairegrandville cabildoÎncă nu există evaluări
- Milieu Therapy / Therapeutic CommunityDocument30 paginiMilieu Therapy / Therapeutic CommunitySaritha SvÎncă nu există evaluări
- Role of Nurses Practitioner in Domestic Violence UMKT 2019Document24 paginiRole of Nurses Practitioner in Domestic Violence UMKT 2019DwiCahyoÎncă nu există evaluări
- Management Theories Hand OutsDocument14 paginiManagement Theories Hand OutsNovelyn PuaÎncă nu există evaluări
- Health Assessment Form FINAL ProjectDocument10 paginiHealth Assessment Form FINAL ProjectClarence AbarratigueÎncă nu există evaluări
- 122 Lecture 1 Milieu TherapyDocument7 pagini122 Lecture 1 Milieu TherapyDENNIS N. MUÑOZÎncă nu există evaluări
- Family Health Nursing PlanDocument2 paginiFamily Health Nursing PlanGuezil Joy R. DelfinÎncă nu există evaluări
- Health AssessmentDocument115 paginiHealth Assessmentteuuuu100% (1)
- Counselling-GATHER ApproachDocument23 paginiCounselling-GATHER ApproachAnilkumar JaraliÎncă nu există evaluări
- Communication For Health EducationDocument58 paginiCommunication For Health EducationBhupendra RohitÎncă nu există evaluări
- Module 2 Implementing Health Education PlanDocument8 paginiModule 2 Implementing Health Education PlanCedrick Mesa Sali-otÎncă nu există evaluări
- Synopsis PPT NomophobiaDocument25 paginiSynopsis PPT NomophobiaRehab KhaleelÎncă nu există evaluări
- What Is Clinical Assessment and Clinical Diagnosis?Document9 paginiWhat Is Clinical Assessment and Clinical Diagnosis?Sunidhi ChaudharyÎncă nu există evaluări
- Application - of - Theory - in - NursingDocument9 paginiApplication - of - Theory - in - Nursingako at ang exo100% (1)
- SUPERVISION-1 NewDocument15 paginiSUPERVISION-1 NewAparna Kingini50% (2)
- Pain Assessment, Reassessment and Management, Grief and Bereavement, End of LIfe CareDocument26 paginiPain Assessment, Reassessment and Management, Grief and Bereavement, End of LIfe Carewilliam turquezaÎncă nu există evaluări
- Data Collection Methods - L ANANDDocument24 paginiData Collection Methods - L ANANDAnand La67% (3)
- C CEF Roles, Character, Team PlainDocument10 paginiC CEF Roles, Character, Team PlainConrad C. CatimbangÎncă nu există evaluări
- Preceptor Evaluation Form Docx CompleteDocument8 paginiPreceptor Evaluation Form Docx Completeapi-279007013Încă nu există evaluări
- Unit 3 Staffing: PlanningDocument10 paginiUnit 3 Staffing: PlanningEeeeeÎncă nu există evaluări
- Telenursing PDFDocument10 paginiTelenursing PDFSujatha J JayabalÎncă nu există evaluări
- Controlling: Reasons For Conducting EvaluationDocument14 paginiControlling: Reasons For Conducting EvaluationAntonio Bejasa JrÎncă nu există evaluări
- On Time Management-NrsDocument24 paginiOn Time Management-NrsIndseti Puducherry50% (2)
- Family Nursing Process - Implementation and Evaluation PDFDocument14 paginiFamily Nursing Process - Implementation and Evaluation PDFms RNÎncă nu există evaluări
- DCLC Therapeutic CommunicationDocument84 paginiDCLC Therapeutic CommunicationlkristinÎncă nu există evaluări
- Code of Ethics:: Presented by Musa Saddam Kiran Mujahid Kiran Saba Minal IrshadDocument16 paginiCode of Ethics:: Presented by Musa Saddam Kiran Mujahid Kiran Saba Minal IrshadAamir100% (1)
- Taking Weight and HeightDocument9 paginiTaking Weight and HeightJennifer WongÎncă nu există evaluări
- Spiritual and PsychosocialDocument40 paginiSpiritual and Psychosocialhaddi awanÎncă nu există evaluări
- Phases of IprDocument3 paginiPhases of Iprvaideeswari kumarÎncă nu există evaluări
- Individual Growth and DevelopmentDocument23 paginiIndividual Growth and DevelopmentSujatha J Jayabal100% (1)
- CBTPDocument30 paginiCBTPDaroo D.TÎncă nu există evaluări
- BFHI Case Studies FINAL PDFDocument61 paginiBFHI Case Studies FINAL PDFYhana Fheb Nabus BayacsanÎncă nu există evaluări
- INTRODUCTION TO GLOBAL HEALTH LessonsDocument39 paginiINTRODUCTION TO GLOBAL HEALTH LessonsDeidra Borus100% (1)
- Cummunity Health Nursing Ii: Study Plan/Checklist (Tal)Document3 paginiCummunity Health Nursing Ii: Study Plan/Checklist (Tal)ライÎncă nu există evaluări
- Hsag Qapi CompanionDocument21 paginiHsag Qapi CompanionAngel Inestroza100% (1)
- POSDCORB - Management Process: PlanningDocument8 paginiPOSDCORB - Management Process: PlanningShannon Dona MassarÎncă nu există evaluări
- Anxiety NCPDocument4 paginiAnxiety NCPMARK JASON DIAZÎncă nu există evaluări
- Performance Evaluation HeadnursingDocument3 paginiPerformance Evaluation HeadnursingBing58Încă nu există evaluări
- Report of Field Visit To National Centre For Disease ControlDocument12 paginiReport of Field Visit To National Centre For Disease ControlVaishali JainarainÎncă nu există evaluări
- Introduction To Community Health NursingDocument23 paginiIntroduction To Community Health NursingAlmasÎncă nu există evaluări
- Modul 6 - Social Diagnosis Assessing Quality of Life ConcernsDocument19 paginiModul 6 - Social Diagnosis Assessing Quality of Life ConcernsKaey NiezamÎncă nu există evaluări
- Theories in CHNDocument61 paginiTheories in CHNkennethÎncă nu există evaluări
- Introduction To Health EducationDocument110 paginiIntroduction To Health EducationRaRe TV100% (1)
- Remodelling of Nola PenderDocument5 paginiRemodelling of Nola PenderDon Chiaw ManongdoÎncă nu există evaluări
- HCD 12203 Basic Medical Microbiology: Click To Edit Master Subtitle StyleDocument16 paginiHCD 12203 Basic Medical Microbiology: Click To Edit Master Subtitle StyleKaey NiezamÎncă nu există evaluări
- Lecture 13 - Case Investigation & Contact TracingDocument20 paginiLecture 13 - Case Investigation & Contact TracingKaey NiezamÎncă nu există evaluări
- Disease EcologyDocument19 paginiDisease EcologyKaey NiezamÎncă nu există evaluări
- Lecture 1 - Introduction To SC CommDocument20 paginiLecture 1 - Introduction To SC CommKaey NiezamÎncă nu există evaluări
- Emerging of Food PathogenDocument51 paginiEmerging of Food PathogenKaey NiezamÎncă nu există evaluări
- Food Spoilage & PreservationDocument37 paginiFood Spoilage & PreservationKaey Niezam100% (2)
- Pest & Vectors Management: Aedes IndexDocument19 paginiPest & Vectors Management: Aedes IndexKaey Niezam100% (5)
- Cleaning & Disinfection 2Document17 paginiCleaning & Disinfection 2Kaey NiezamÎncă nu există evaluări
- Training & Education of Food HandlersDocument24 paginiTraining & Education of Food HandlersKaey Niezam100% (1)
- Personal HygieneDocument30 paginiPersonal HygieneKaey NiezamÎncă nu există evaluări
- Cleaning & DisinfectionDocument22 paginiCleaning & DisinfectionKaey NiezamÎncă nu există evaluări
- Topic 2 - Theory & Principle of Disease 2Document22 paginiTopic 2 - Theory & Principle of Disease 2Kaey NiezamÎncă nu există evaluări
- Topic 3 - Disease Control StrategiesDocument25 paginiTopic 3 - Disease Control StrategiesKaey NiezamÎncă nu există evaluări
- Modul 9 - Selection of Educational StrategiesDocument26 paginiModul 9 - Selection of Educational StrategiesKaey NiezamÎncă nu există evaluări
- Modul 5 - Health Promotion PlanningDocument34 paginiModul 5 - Health Promotion PlanningKaey NiezamÎncă nu există evaluări
- Topic 1 - Theory & Principle of DiseaseDocument15 paginiTopic 1 - Theory & Principle of DiseaseKaey NiezamÎncă nu există evaluări
- Modul 8 - Education DiagnosisDocument18 paginiModul 8 - Education DiagnosisKaey NiezamÎncă nu există evaluări
- Modul 6 - Social Diagnosis Assessing Quality of Life ConcernsDocument19 paginiModul 6 - Social Diagnosis Assessing Quality of Life ConcernsKaey NiezamÎncă nu există evaluări
- Modul 4 - Theory and Pronciple of Health EducationDocument16 paginiModul 4 - Theory and Pronciple of Health EducationKaey NiezamÎncă nu există evaluări
- LipoproteinDocument12 paginiLipoproteinridho azha100% (2)
- English Ass EssayDocument5 paginiEnglish Ass EssayEllen TingÎncă nu există evaluări
- Document (4) FNCP PrioritizationDocument7 paginiDocument (4) FNCP Prioritizationrose angelaÎncă nu există evaluări
- learningDataStoreALTICOR PRODLearningdata20221016 225016 5262assetsdocsXS Ignite EN PDFDocument32 paginilearningDataStoreALTICOR PRODLearningdata20221016 225016 5262assetsdocsXS Ignite EN PDFThamarai ThamodharanÎncă nu există evaluări
- TNT Get Back in Shape Workouts PDFDocument10 paginiTNT Get Back in Shape Workouts PDFaboubakereldjazairi100% (1)
- Urban KryptoniteDocument196 paginiUrban KryptoniteJerome Love67% (3)
- Anatomy MnemonicsDocument46 paginiAnatomy MnemonicsMini ManraiÎncă nu există evaluări
- Metabical: Pricing, Packaging, and Demand Forecasting For A New Weight-Loss DrugDocument4 paginiMetabical: Pricing, Packaging, and Demand Forecasting For A New Weight-Loss DrugKishan BhalotiyaÎncă nu există evaluări
- Fooducate Worksheet 2012-08-14 MathDocument5 paginiFooducate Worksheet 2012-08-14 Mathapi-26400457150% (4)
- 50 Ways To HealDocument12 pagini50 Ways To HealBrooke PenaÎncă nu există evaluări
- CKD CHCRTDocument28 paginiCKD CHCRTNurhidayati KeriyunÎncă nu există evaluări
- BMI Age Percentiles GIRLSDocument1 paginăBMI Age Percentiles GIRLSEric Grossi MoratoÎncă nu există evaluări
- Junk Food Consumption Awareness and Its Health ConDocument6 paginiJunk Food Consumption Awareness and Its Health Concristine borjaÎncă nu există evaluări
- Neuro MassDocument3 paginiNeuro MassPete PuzaÎncă nu există evaluări
- Biochemical Profile of Albino Rats With Experimentally Induced Metabolic Syndrome...Document11 paginiBiochemical Profile of Albino Rats With Experimentally Induced Metabolic Syndrome...Chiemekam Samuel EzechukwuÎncă nu există evaluări
- Prescription of Exercise For Health and FitnessDocument27 paginiPrescription of Exercise For Health and FitnessedelinÎncă nu există evaluări
- Gut Dysfunction and Non-Alcoholic Fatty Liver DiseaseDocument9 paginiGut Dysfunction and Non-Alcoholic Fatty Liver DiseaseAshwiniÎncă nu există evaluări
- 20 Bodybuilding Secrets You Won T Find On Google MPMD 3 PDFDocument35 pagini20 Bodybuilding Secrets You Won T Find On Google MPMD 3 PDFbobÎncă nu există evaluări
- Women's Health & Fitness - February 2016 AU PDFDocument124 paginiWomen's Health & Fitness - February 2016 AU PDFCatalin MunteanuÎncă nu există evaluări
- Oral Presentation Order NewDocument16 paginiOral Presentation Order NewNovel WidyaÎncă nu există evaluări
- Basic Diabetes EducationDocument73 paginiBasic Diabetes EducationDr DiabeatÎncă nu există evaluări
- Top 200 Sorted by Drug ClassDocument3 paginiTop 200 Sorted by Drug Classthompjo2394100% (7)
- Prevention and Management of Diabetic Foot Ulcers PDFDocument68 paginiPrevention and Management of Diabetic Foot Ulcers PDFJianhua Shi100% (2)
- Jingky CaseDocument8 paginiJingky CaseLouie Jay DelBarrio LlenoÎncă nu există evaluări
- Complication & Failure of ImplantsDocument82 paginiComplication & Failure of ImplantsDrIbrahimShaikhÎncă nu există evaluări
- A Developing Self-Management SkillsDocument11 paginiA Developing Self-Management Skillsjjespiritu21Încă nu există evaluări
- CardiologyDocument62 paginiCardiologyLaura Kathrine Simpson92% (12)
- FNCPDocument4 paginiFNCPJonalyn Tumanguil100% (2)
- Fast Food AddictionDocument14 paginiFast Food AddictionHana Renoblas0% (2)
- Àcidez en Grasa Metodo General 02-01aDocument2 paginiÀcidez en Grasa Metodo General 02-01aSarah Wells100% (1)