S-ar putea să vă placă și
- FileChapter 2 Philosophical PerspectivesDocument21 paginiFileChapter 2 Philosophical PerspectivesMai SenaninÎncă nu există evaluări
- Levinas PowerpointDocument14 paginiLevinas PowerpointMai SenaninÎncă nu există evaluări
- FaceDocument3 paginiFaceMai SenaninÎncă nu există evaluări
- CaringDocument16 paginiCaringPurwadi SujalmoÎncă nu există evaluări
- Caring in NursingDocument12 paginiCaring in NursingMai SenaninÎncă nu există evaluări
- Caring in NursingDocument12 paginiCaring in NursingMai SenaninÎncă nu există evaluări
- FaceDocument3 paginiFaceMai SenaninÎncă nu există evaluări
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (890)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (587)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (72)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (119)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Production and Export of GrapesDocument64 paginiProduction and Export of GrapesYogesh Bijwe100% (2)
- Homemade Cinnamon Rolls PDFDocument3 paginiHomemade Cinnamon Rolls PDFSalma MohsenÎncă nu există evaluări
- The Hillgate Pub MenuDocument1 paginăThe Hillgate Pub MenuKinvara CorbettÎncă nu există evaluări
- Wedding Package: Emerald - Saphire - RubyDocument2 paginiWedding Package: Emerald - Saphire - RubypurwantihandayaniÎncă nu există evaluări
- New Frontiers 3 WB Transcripts PDFDocument22 paginiNew Frontiers 3 WB Transcripts PDFjose osorio olvera del 3 D NUM 32Încă nu există evaluări
- Environmental Issues DraftDocument21 paginiEnvironmental Issues DraftPranav Pratap SinghÎncă nu există evaluări
- BCG & SWOT Parle Products Private Limited - GST and Retaining CompetitivenessDocument12 paginiBCG & SWOT Parle Products Private Limited - GST and Retaining Competitivenessritesh raiÎncă nu există evaluări
- Core design principles and tenets of permacultureDocument4 paginiCore design principles and tenets of permacultureTdisÎncă nu există evaluări
- Culture and SocietyDocument23 paginiCulture and SocietyGlecy RazÎncă nu există evaluări
- G.D. Goenka Public School: Investigatory ProjectDocument20 paginiG.D. Goenka Public School: Investigatory ProjectVansh GuptaÎncă nu există evaluări
- KFC Delivery Menu in SIngaporeDocument1 paginăKFC Delivery Menu in SIngaporedmlawrenceÎncă nu există evaluări
- 2018-2019 Vào 10 Chuyên H Chí Minh - AnswerDocument10 pagini2018-2019 Vào 10 Chuyên H Chí Minh - AnswerTrang100% (1)
- YAO Menu (All) PDFDocument6 paginiYAO Menu (All) PDFINGODWETRUST79Încă nu există evaluări
- Guar Gum MachineryDocument14 paginiGuar Gum MachinerySundaresanÎncă nu există evaluări
- EMRAC EngineeringDocument12 paginiEMRAC EngineeringAnonymous QSLV4dNÎncă nu există evaluări
- Star Alliance Timetable 2004Document211 paginiStar Alliance Timetable 2004yoshifunky93Încă nu există evaluări
- Papa No Iu Koto Wo Kikinasai, Vol.1Document293 paginiPapa No Iu Koto Wo Kikinasai, Vol.1Tiana MampiononaÎncă nu există evaluări
- The Agraria: An Agricultural and Environmental e - MagazineDocument34 paginiThe Agraria: An Agricultural and Environmental e - MagazineVaibhav DafaleÎncă nu există evaluări
- Trizara Pricelist 2018Document15 paginiTrizara Pricelist 2018Handiani PandansariÎncă nu există evaluări
- Refrigeration: From Wikipedia, The Free EncyclopediaDocument14 paginiRefrigeration: From Wikipedia, The Free Encyclopediaayan1688Încă nu există evaluări
- Easy 30-Minute Tiramisu RecipeDocument3 paginiEasy 30-Minute Tiramisu Recipesara gomezÎncă nu există evaluări
- 1-2019-History of Bar Service IndustryDocument36 pagini1-2019-History of Bar Service IndustryAaron Castro100% (2)
- The Croods - Lessons (Final)Document54 paginiThe Croods - Lessons (Final)Khun Win MaungÎncă nu există evaluări
- Vietnam Formula Milk Market StudyDocument55 paginiVietnam Formula Milk Market StudyNgo Thi OanhÎncă nu există evaluări
- CXS - 052e Capsuni Congelate PDFDocument6 paginiCXS - 052e Capsuni Congelate PDFdorinutza280Încă nu există evaluări
- 16 Tenses Passive Voice ExamplesDocument3 pagini16 Tenses Passive Voice Examplesbudi putraÎncă nu există evaluări
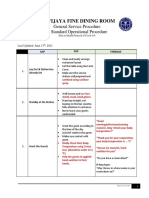
- Fine Dining Restaurant GSP & SOP - Due To Covid19 Health Protocol - June 2021Document9 paginiFine Dining Restaurant GSP & SOP - Due To Covid19 Health Protocol - June 2021Edo HadiÎncă nu există evaluări
- Who Wants To Be A Millionaire PowerPointDocument54 paginiWho Wants To Be A Millionaire PowerPointTsheba Marie F. BandojoÎncă nu există evaluări
- Dietary Guidelines For A Healthy Postnatal DietDocument4 paginiDietary Guidelines For A Healthy Postnatal Dietcheyong100% (1)
- Finding A Sustainable Food System For ManchesterDocument115 paginiFinding A Sustainable Food System For ManchesterThe Kindling Trust.Încă nu există evaluări