S-ar putea să vă placă și
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Civilian Commando PDFDocument111 paginiCivilian Commando PDFHankWolfe100% (3)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Plumbing Practice ExamDocument16 paginiPlumbing Practice Examharold_bhie100% (2)
- Mythic Masters MagazineDocument38 paginiMythic Masters Magazineucpap100% (2)
- Physiology of LactationDocument29 paginiPhysiology of Lactationcorzpun16867879% (14)
- Grooming Assignment Assessor:-Presented By: - Batch: - YearDocument29 paginiGrooming Assignment Assessor:-Presented By: - Batch: - YearSAURABH KUMARÎncă nu există evaluări
- Japanese Grammar FocusDocument222 paginiJapanese Grammar FocusLucas MachadoÎncă nu există evaluări
- Re Lactation and Induced LactationDocument34 paginiRe Lactation and Induced Lactationcorzpun168678100% (2)
- Our Qualifications As Mentors: Actual Experience in Retail Business Management 10 YearsDocument86 paginiOur Qualifications As Mentors: Actual Experience in Retail Business Management 10 YearsDothy TumÎncă nu există evaluări
- AO - MBFHI. 2pptDocument44 paginiAO - MBFHI. 2pptcorzpun168678100% (3)
- E.O. 51 and RIRRDocument29 paginiE.O. 51 and RIRRcorzpun168678100% (6)
- Folleto+extraible+guía+del+pisco+2021 CompressedDocument32 paginiFolleto+extraible+guía+del+pisco+2021 CompressedGonzalo Arias R.Încă nu există evaluări
- Human Milk BankDocument29 paginiHuman Milk Bankcorzpun168678100% (1)
- Republic Act 7600Document10 paginiRepublic Act 7600corzpun168678100% (5)
- Patrick John Mejia PunsalangDocument2 paginiPatrick John Mejia Punsalangcorzpun168678Încă nu există evaluări
- Maternal and Child SeparationDocument40 paginiMaternal and Child Separationcorzpun168678Încă nu există evaluări
- Drugs in LactationDocument36 paginiDrugs in Lactationcorzpun168678100% (1)
- Common Maternal Breastfeeding ProblemsDocument49 paginiCommon Maternal Breastfeeding Problemscorzpun168678Încă nu există evaluări
- Bedlam BoyzDocument149 paginiBedlam BoyzbruersmÎncă nu există evaluări
- Documents - Tips Exam Form 1 English Pt3 FormatDocument5 paginiDocuments - Tips Exam Form 1 English Pt3 FormatDato Habil Azman100% (1)
- Cuktura de BelgicaDocument9 paginiCuktura de BelgicaMaria Julia MartinezÎncă nu există evaluări
- Take On SingkawangDocument4 paginiTake On SingkawangTeuku Benladin HakimÎncă nu există evaluări
- Art of MixingDocument13 paginiArt of MixingChristian Alejandrino100% (1)
- 'Used To' For Past HabitsDocument13 pagini'Used To' For Past HabitsYaina IvanovaÎncă nu există evaluări
- Legal Ethics ProjectDocument44 paginiLegal Ethics ProjectKartik SharmaÎncă nu există evaluări
- Why A Calorie Deficit Is Key To Effective Weight Loss by Steve SearleDocument8 paginiWhy A Calorie Deficit Is Key To Effective Weight Loss by Steve SearlesearlsaÎncă nu există evaluări
- TM Comply With Workplace Hygiene Proc 310812 PDFDocument100 paginiTM Comply With Workplace Hygiene Proc 310812 PDFCecilleMananitaÎncă nu există evaluări
- Marvel Tea ProfileDocument5 paginiMarvel Tea ProfilePrateek SaxenaÎncă nu există evaluări
- English 3 Reading Nat 1Document23 paginiEnglish 3 Reading Nat 1robelynemendoza17Încă nu există evaluări
- Asian PaintsDocument20 paginiAsian PaintsSubhojit Roy100% (1)
- Calculo de PH Agua Cervejeira English IPADocument4 paginiCalculo de PH Agua Cervejeira English IPAFrederico Luiz de SáÎncă nu există evaluări
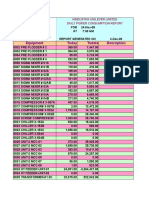
- Equipment Today Todate Description: Hindustan Unilever Limited Daily Power Consumption ReportDocument2 paginiEquipment Today Todate Description: Hindustan Unilever Limited Daily Power Consumption Reportcity1212Încă nu există evaluări
- Nursing Care in RadiotherapyDocument26 paginiNursing Care in Radiotherapyحسام جبار مجيد100% (1)
- Introduction To Alcoholic BeveragesDocument2 paginiIntroduction To Alcoholic BeveragesRHTi BDÎncă nu există evaluări
- Linteloo MeubelenDocument98 paginiLinteloo MeubelenWilfred Stegeman100% (3)
- Void ReturDocument30 paginiVoid ReturSakya Kumara JatiÎncă nu există evaluări
- Budapest Survival KitDocument64 paginiBudapest Survival Kitd-fbuser-22759885Încă nu există evaluări
- The Testimonial: October 2009Document15 paginiThe Testimonial: October 2009api-26017242Încă nu există evaluări
- Ordaz Alli 79418 Assignment3Document7 paginiOrdaz Alli 79418 Assignment3api-265450712Încă nu există evaluări
- Sample Thesis About Coffee ShopDocument6 paginiSample Thesis About Coffee Shopdwt65fcw100% (2)
- Bakery Review Feb-March 2019 Issue. Reach 9810315463 To Advertise or Subscribe ! PDFDocument52 paginiBakery Review Feb-March 2019 Issue. Reach 9810315463 To Advertise or Subscribe ! PDFAmreesh MisraÎncă nu există evaluări