S-ar putea să vă placă și
- Differential DiagnosisDocument28 paginiDifferential DiagnosisDr. Khawer BaigÎncă nu există evaluări
- Shortened REM Latency and Increased REM: Previous AttemptDocument19 paginiShortened REM Latency and Increased REM: Previous AttemptActeen MyoseenÎncă nu există evaluări
- Telemental Health: Clinical, Technical, and Administrative Foundations for Evidence-Based PracticeDe la EverandTelemental Health: Clinical, Technical, and Administrative Foundations for Evidence-Based PracticeÎncă nu există evaluări
- AIMS. Scales-Abnormal-Involuntary-Movement-Scale PDFDocument2 paginiAIMS. Scales-Abnormal-Involuntary-Movement-Scale PDFVictoria RomeroÎncă nu există evaluări
- Psych Final BlueprintDocument10 paginiPsych Final BlueprintGrace LivingstonÎncă nu există evaluări
- Pharmacology - (5) Psychotic DrugsDocument8 paginiPharmacology - (5) Psychotic DrugsSamantha DiegoÎncă nu există evaluări
- Fig psychiatricAssessmentFormDocument4 paginiFig psychiatricAssessmentFormabbey jane mallillin100% (1)
- HPI GuidelinesDocument5 paginiHPI GuidelinesHani NadiahÎncă nu există evaluări
- PsychotropicsDocument4 paginiPsychotropicsGeoffrey KernsÎncă nu există evaluări
- Final Capstone PaperDocument15 paginiFinal Capstone Paperapi-478784238Încă nu există evaluări
- PMHNP Case Study Diagnosis and TreatmentDocument7 paginiPMHNP Case Study Diagnosis and TreatmentSoumyadeep BoseÎncă nu există evaluări
- PsychiatryDocument92 paginiPsychiatrykimÎncă nu există evaluări
- PSYC - Medication TemplateDocument15 paginiPSYC - Medication TemplateM Henry100% (1)
- The Wiley-Blackwell Handbook of Addiction PsychopharmacologyDe la EverandThe Wiley-Blackwell Handbook of Addiction PsychopharmacologyÎncă nu există evaluări
- Mental StatusDocument6 paginiMental StatusIgor Oliveira100% (1)
- Practical Psychopharmacology in Children and Adolescents: Anoop Vermani MD Fellow, Child and Adolescent PsychiatryDocument29 paginiPractical Psychopharmacology in Children and Adolescents: Anoop Vermani MD Fellow, Child and Adolescent PsychiatryShahinaz ShamsÎncă nu există evaluări
- Mental Status Examination Rapid Record Form: CatatoniaDocument3 paginiMental Status Examination Rapid Record Form: CatatoniaNicole TangcoÎncă nu există evaluări
- Psych-CLEAR: Psychopathology Made Clear and EasyDocument31 paginiPsych-CLEAR: Psychopathology Made Clear and EasynurulÎncă nu există evaluări
- Template For Clinical Progress Note June 2009Document3 paginiTemplate For Clinical Progress Note June 2009Buthaina AltenaijiÎncă nu există evaluări
- The Massachusetts General Hospital Textbook on Diversity and Cultural Sensitivity in Mental HealthDe la EverandThe Massachusetts General Hospital Textbook on Diversity and Cultural Sensitivity in Mental HealthÎncă nu există evaluări
- Test 2 222Document12 paginiTest 2 222Ken Carter0% (1)
- 1.psychiatric Neuroscience - Incorporating Pathophysiology Into Clinical Case Formulation - ClinicalKeyDocument43 pagini1.psychiatric Neuroscience - Incorporating Pathophysiology Into Clinical Case Formulation - ClinicalKeyClaudia0% (1)
- Sample Case Study For DMS-IV-TRDocument6 paginiSample Case Study For DMS-IV-TRohphooeyÎncă nu există evaluări
- Understanding Psychiatric History Taking and Mental Status ExaminationDocument56 paginiUnderstanding Psychiatric History Taking and Mental Status ExaminationHardeep KaurÎncă nu există evaluări
- Psychiatry Practice BoostersDe la EverandPsychiatry Practice BoostersJesse KoskeyÎncă nu există evaluări
- History Taking and Mental State Exam for PsychosisDocument10 paginiHistory Taking and Mental State Exam for PsychosisNathan T. CheungÎncă nu există evaluări
- Biomarkers and Mental Illness: It’s Not All in the MindDe la EverandBiomarkers and Mental Illness: It’s Not All in the MindÎncă nu există evaluări
- Psychiatry history taking and case formulation templateDocument11 paginiPsychiatry history taking and case formulation templateNicholasÎncă nu există evaluări
- Disorders of ThoughtDocument22 paginiDisorders of ThoughtMohammad Farouq OmarÎncă nu există evaluări
- Racism and Psychiatry: Contemporary Issues and InterventionsDe la EverandRacism and Psychiatry: Contemporary Issues and InterventionsMorgan M. MedlockÎncă nu există evaluări
- Psych Meds - Good Reference CardDocument2 paginiPsych Meds - Good Reference Cardwin100% (1)
- Laboratory Testing in PsychiatryDocument29 paginiLaboratory Testing in PsychiatrySera ChunÎncă nu există evaluări
- PsychopharmacologyDocument49 paginiPsychopharmacologysazaki224Încă nu există evaluări
- Exam 1 2Document18 paginiExam 1 2api-444187370Încă nu există evaluări
- AMBULATORY WOMEN'S HEALTH CARE NURSING: Passbooks Study GuideDe la EverandAMBULATORY WOMEN'S HEALTH CARE NURSING: Passbooks Study GuideÎncă nu există evaluări
- Ideal Inpatient Progress Notes Template of Ideal Progress NoteDocument2 paginiIdeal Inpatient Progress Notes Template of Ideal Progress Notebrianzfl100% (1)
- Varcarolis CH 1Document21 paginiVarcarolis CH 1Catlyn ChatpmanÎncă nu există evaluări
- Patient Write-Up Example 2Document6 paginiPatient Write-Up Example 2Meliara101Încă nu există evaluări
- Clinical Guidelines and Care ProtocolsDe la EverandClinical Guidelines and Care ProtocolsEvaluare: 5 din 5 stele5/5 (1)
- Emergency Psychiatry: Care in Special SettingsDocument15 paginiEmergency Psychiatry: Care in Special SettingsCassandra BoduchÎncă nu există evaluări
- Mental Status ExamDocument7 paginiMental Status ExamDanielle BanÎncă nu există evaluări
- Cognitive Behavioral Psychopharmacology: The Clinical Practice of Evidence-Based Biopsychosocial IntegrationDe la EverandCognitive Behavioral Psychopharmacology: The Clinical Practice of Evidence-Based Biopsychosocial IntegrationMark MuseÎncă nu există evaluări
- Psychiatry Capstone 43020 Agitation PsychopharmacologyDocument20 paginiPsychiatry Capstone 43020 Agitation Psychopharmacologyapi-552282470Încă nu există evaluări
- Anxiety DisordersDocument14 paginiAnxiety DisordersAlex BorroelÎncă nu există evaluări
- QTC Flow Diagram With Medications Final Dec 17 A3 With LogosDocument1 paginăQTC Flow Diagram With Medications Final Dec 17 A3 With LogosMelissa MurilloÎncă nu există evaluări
- Case Management Frameworks A Complete Guide - 2019 EditionDe la EverandCase Management Frameworks A Complete Guide - 2019 EditionÎncă nu există evaluări
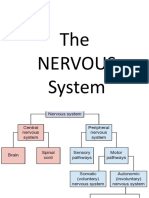
- The BrainDocument22 paginiThe BrainClae NapiÎncă nu există evaluări
- Brain, Behavior & PsychopharmacologyDocument42 paginiBrain, Behavior & PsychopharmacologyRichky Nurhakim100% (4)
- Rutter's Child and Adolescent Psychiatry PDF - Căutare GoogleDocument1 paginăRutter's Child and Adolescent Psychiatry PDF - Căutare GoogleMihaela EvaÎncă nu există evaluări
- Patient Progress Note ProtocolDocument8 paginiPatient Progress Note ProtocolVito Wilfredo100% (1)
- Sudden Onset (Within 2 Weeks) of at Least One of TheDocument2 paginiSudden Onset (Within 2 Weeks) of at Least One of TheNeicole BandalaÎncă nu există evaluări
- Ab Psych - NotesDocument27 paginiAb Psych - NotesStars NKLÎncă nu există evaluări
- Suicidality Assessment and Documentation For Healthcare ProvidersDocument179 paginiSuicidality Assessment and Documentation For Healthcare ProvidersFrancisco LatorreÎncă nu există evaluări
- Case History, MSE and Rating Scales - in Psychological AssessmentDocument29 paginiCase History, MSE and Rating Scales - in Psychological Assessmentsu84Încă nu există evaluări
- Case Presentation StyleDocument7 paginiCase Presentation StyleNiteshSinghÎncă nu există evaluări
- Mental Status Exam ChecklistDocument5 paginiMental Status Exam ChecklistTauqeer AhmedÎncă nu există evaluări
- Case-Anheuser Busch UpdatedDocument12 paginiCase-Anheuser Busch UpdatedJennifer Bello Araquel100% (1)
- Activity Relationship Chart 2Document2 paginiActivity Relationship Chart 2Yugi SupriatnaÎncă nu există evaluări
- Skill 6 (Coordinate Connector)Document12 paginiSkill 6 (Coordinate Connector)Yugi SupriatnaÎncă nu există evaluări
- Modul 1 - Forecasting PDFDocument3 paginiModul 1 - Forecasting PDFYugi SupriatnaÎncă nu există evaluări
- Writing Task 2 - Answer The Question PDFDocument4 paginiWriting Task 2 - Answer The Question PDFYugi SupriatnaÎncă nu există evaluări
- IELTS Writing Lesson Plan 1Document10 paginiIELTS Writing Lesson Plan 1Alice Starkey100% (1)
- IELTS Writing Lesson Plan 5Document15 paginiIELTS Writing Lesson Plan 5Trang Nguyen ThuÎncă nu există evaluări
- IELTS Writing Lesson Plan 1 PDFDocument10 paginiIELTS Writing Lesson Plan 1 PDFYugi SupriatnaÎncă nu există evaluări
- IELTS Writing Lesson Plan 5Document15 paginiIELTS Writing Lesson Plan 5Trang Nguyen ThuÎncă nu există evaluări
- Clause (Adjective+Adverb)Document13 paginiClause (Adjective+Adverb)Yugi Supriatna100% (1)
- Permanently Activate Microsoft Office Professional Plus 2010Document1 paginăPermanently Activate Microsoft Office Professional Plus 2010kaifiahmed76% (21)
- IELTS Writing Lesson Plan 2 PDFDocument12 paginiIELTS Writing Lesson Plan 2 PDFYugi Supriatna0% (1)
- Prosedure Tune Up (HC Eng)Document19 paginiProsedure Tune Up (HC Eng)Yugi SupriatnaÎncă nu există evaluări
- Mech 203 Auto Differential Transmission ProjectDocument29 paginiMech 203 Auto Differential Transmission ProjectYugi SupriatnaÎncă nu există evaluări
- Depression Diagnostic Criteria and Severity RatingDocument1 paginăDepression Diagnostic Criteria and Severity Ratingapi-310299713Încă nu există evaluări
- Post-Stroke Movement Disorders The Clinical Neuroanatomic and Demographic Portrait of 284 Published CasesDocument10 paginiPost-Stroke Movement Disorders The Clinical Neuroanatomic and Demographic Portrait of 284 Published CaseskhaeejahÎncă nu există evaluări
- Counseling Case Report Smoking Cigarette 6381 - RepairedDocument5 paginiCounseling Case Report Smoking Cigarette 6381 - RepairedSahil MushafÎncă nu există evaluări
- Prenatal Care Assessment: Monitoring Risks and ComplicationsDocument6 paginiPrenatal Care Assessment: Monitoring Risks and ComplicationsSupremo Manuel M DeluaoÎncă nu există evaluări
- Hemifacial SpasmDocument4 paginiHemifacial Spasmyeddika12Încă nu există evaluări
- Depression - PresentationDocument12 paginiDepression - PresentationAmeera Masud LoneÎncă nu există evaluări
- Dass-21 Scoring Online Percentiles Calculator v2Document3 paginiDass-21 Scoring Online Percentiles Calculator v2Irhamna IirÎncă nu există evaluări
- Depression PresentationDocument12 paginiDepression PresentationYitzRichmond100% (1)
- Management of Benzodiazepine Misuse and Dependence: Jonathan Brett Bridin MurnionDocument4 paginiManagement of Benzodiazepine Misuse and Dependence: Jonathan Brett Bridin MurnionLucius MarpleÎncă nu există evaluări
- Anxiety Disorders: Presented byDocument38 paginiAnxiety Disorders: Presented byRudra prasad Sahu100% (1)
- DKA Diagnosis and TreatmentDocument16 paginiDKA Diagnosis and TreatmentDina M ElbakaryÎncă nu există evaluări
- Child Health NursingDocument5 paginiChild Health Nursingprincipalnursing rampurhat 2023Încă nu există evaluări
- Client Intake Form SEODocument6 paginiClient Intake Form SEOAiman RashidÎncă nu există evaluări
- Neonatal SeizuresDocument4 paginiNeonatal SeizuresSerag EdeenÎncă nu există evaluări
- Antepartum HemorrhageDocument52 paginiAntepartum HemorrhageKomalah ChenasammyÎncă nu există evaluări
- Achmad Fitrah Khalid JCUDocument1 paginăAchmad Fitrah Khalid JCUArmadilloo CorpÎncă nu există evaluări
- Rawatan Klien Dua DiagnosisDocument62 paginiRawatan Klien Dua DiagnosisPUSAT LATIHAN AADKÎncă nu există evaluări
- Benzo Withdrawal SyndromeDocument7 paginiBenzo Withdrawal SyndromeWernerÎncă nu există evaluări
- B.ing - M.fadhel Syah Al Bukhori - G1a118144Document7 paginiB.ing - M.fadhel Syah Al Bukhori - G1a118144mufasyahÎncă nu există evaluări
- Psychiatric Evaluation ReportDocument5 paginiPsychiatric Evaluation Reportwafaa alwafiÎncă nu există evaluări
- Neurological Observations Chart (NOCDocument2 paginiNeurological Observations Chart (NOCJamaica Limejuice100% (1)
- Fasting in The Treatment of Diabetes and High Blood PressureDocument2 paginiFasting in The Treatment of Diabetes and High Blood PressureTrueNorth Health Center100% (1)
- Traumatic Brain Injury Final 2013.5.29Document59 paginiTraumatic Brain Injury Final 2013.5.29asylum1968Încă nu există evaluări
- Jurnal Psikiatri 6Document8 paginiJurnal Psikiatri 6Dati DelianaÎncă nu există evaluări
- System Broken: How Public Drug Coverage Is Failing Canadians With Mental Illness"Document25 paginiSystem Broken: How Public Drug Coverage Is Failing Canadians With Mental Illness"CityNewsTorontoÎncă nu există evaluări
- Mental Illness in Third World Countries - An Overview.Document20 paginiMental Illness in Third World Countries - An Overview.Cherif100% (1)
- Drug Addiction TreatmentDocument12 paginiDrug Addiction TreatmentDanny WindhamÎncă nu există evaluări
- Gabapentin medication guideDocument2 paginiGabapentin medication guideLucia VillavicencioÎncă nu există evaluări
- Genetic disorders from meiotic errorsDocument1 paginăGenetic disorders from meiotic errorsJayrelle D. SafranÎncă nu există evaluări
- Neurology Board ReviewDocument16 paginiNeurology Board ReviewNabeel Kouka, MD, DO, MBA, MPH67% (3)