S-ar putea să vă placă și
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (120)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- AHA ACLS Megacode ScenariosDocument6 paginiAHA ACLS Megacode ScenariosVitor Hugo G Correia86% (7)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Angina Pectoris Nursing Care PlanDocument1 paginăAngina Pectoris Nursing Care PlanjamieboyRN86% (7)
- Pass PACES in Single AttemptDocument101 paginiPass PACES in Single AttemptSOMNATHÎncă nu există evaluări
- Module 2 Case Study StudentfDocument4 paginiModule 2 Case Study Studentfapi-675875543Încă nu există evaluări
- Resident/Fellow Member Application: CodeDocument2 paginiResident/Fellow Member Application: CodeKavya ShreeÎncă nu există evaluări
- Acyanitic DefectsDocument9 paginiAcyanitic DefectsHalla BennaaÎncă nu există evaluări
- 5 ECG Changes of Hyperkalemia You Need To Know: 1. Tall 'Tented' T WavesDocument4 pagini5 ECG Changes of Hyperkalemia You Need To Know: 1. Tall 'Tented' T Wavesricky hutagalungÎncă nu există evaluări
- Medical-Surgical Management For RHDDocument4 paginiMedical-Surgical Management For RHDJansen Arquilita RiveraÎncă nu există evaluări
- Tetralogy of Fallot: Cyanotic Congenital Heart DiseaseDocument31 paginiTetralogy of Fallot: Cyanotic Congenital Heart DiseaseJabir EspinaÎncă nu există evaluări
- 3 Combined AHA BLS ACLS Updates CombinedDocument5 pagini3 Combined AHA BLS ACLS Updates Combinedamanrup randhawa100% (1)
- Impact Factor - A Valid Measure of Journal QualityDocument5 paginiImpact Factor - A Valid Measure of Journal QualityuzairafzalÎncă nu există evaluări
- Etiqa Accredited Doctors As of 012323Document2.862 paginiEtiqa Accredited Doctors As of 012323madel gardoseÎncă nu există evaluări
- Laporan Rsisa JilidDocument16 paginiLaporan Rsisa JilidGinaÎncă nu există evaluări
- Acls Study Guide 2016Document2 paginiAcls Study Guide 2016Caridad RodasÎncă nu există evaluări
- Sample of Clinical PortraitDocument3 paginiSample of Clinical PortraitSweetie StarÎncă nu există evaluări
- Clinica Especialidades San Judas Tadeo Ecg Holter Report: Print Time:2022-10-01 10:33:53Document6 paginiClinica Especialidades San Judas Tadeo Ecg Holter Report: Print Time:2022-10-01 10:33:53Agustin Fau MaravillaÎncă nu există evaluări
- Hafiz Abdul Rehman (1) - CompressedDocument1 paginăHafiz Abdul Rehman (1) - CompressedFaisal BasharatÎncă nu există evaluări
- Cardiorenal Syndrome Definition, Prevalence, Diagnosis and PathophysiologyDocument18 paginiCardiorenal Syndrome Definition, Prevalence, Diagnosis and PathophysiologyfelipetheÎncă nu există evaluări
- 1 s2.0 S2772930322004367 MainDocument15 pagini1 s2.0 S2772930322004367 MainVimal NishadÎncă nu există evaluări
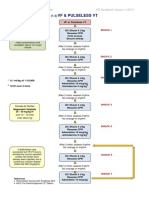
- VF & Pulseless VTDocument1 paginăVF & Pulseless VTmadimadi11Încă nu există evaluări
- Factors Affecting Chronic Kidney DiseaseDocument6 paginiFactors Affecting Chronic Kidney DiseaseUpitFlowÎncă nu există evaluări
- 10 1016@j Biombioe 2020 105881Document1 pagină10 1016@j Biombioe 2020 105881Alex SmithÎncă nu există evaluări
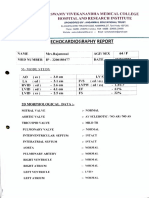
- ECOCARDIODocument3 paginiECOCARDIOArun ComedsÎncă nu există evaluări
- Cronic Heart Failure - EscDocument55 paginiCronic Heart Failure - EscRisti Graharti100% (1)
- Sinus Brad, Tach, PAC, PVCDocument17 paginiSinus Brad, Tach, PAC, PVCEdRobertArnadÎncă nu există evaluări
- Acyanotic Congenital Heart Disease: Pediatric Cardiology Division University of Sumatera UtaraDocument40 paginiAcyanotic Congenital Heart Disease: Pediatric Cardiology Division University of Sumatera UtaraHanda YaniÎncă nu există evaluări
- History of AEDs Saves LivesDocument13 paginiHistory of AEDs Saves LivesAdam ProkopchukÎncă nu există evaluări
- PlabDocument214 paginiPlabKarata SinghÎncă nu există evaluări
- 2015 Akutni Koronarni SindromDocument98 pagini2015 Akutni Koronarni SindromIvanMihailovicÎncă nu există evaluări
- Comprehensive Clinical Nephrology 6Th Edition John Feehally full chapterDocument51 paginiComprehensive Clinical Nephrology 6Th Edition John Feehally full chaptercynthia.casey475100% (13)