S-ar putea să vă placă și
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- 12 Uronic Acid PathwayDocument21 pagini12 Uronic Acid PathwayAnand VeerananÎncă nu există evaluări
- Integrated Metabolism - 080144Document25 paginiIntegrated Metabolism - 080144Anand VeerananÎncă nu există evaluări
- Cell & Membrane Transport-1-3 - 091256Document138 paginiCell & Membrane Transport-1-3 - 091256Anand VeerananÎncă nu există evaluări
- Vitamin B12Document80 paginiVitamin B12Anand Veeranan100% (1)
- 12 Monosaccharide METABOLISMDocument72 pagini12 Monosaccharide METABOLISMAnand VeerananÎncă nu există evaluări
- 12 Fructose MetabolismDocument61 pagini12 Fructose MetabolismAnand Veeranan100% (1)
- Estimation of AlbuminDocument2 paginiEstimation of AlbuminAnand VeerananÎncă nu există evaluări
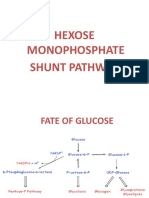
- Hexose Monophosphate Shunt PathwayDocument45 paginiHexose Monophosphate Shunt PathwayAnand VeerananÎncă nu există evaluări
- 9 Regulation of Blood GlucoseDocument47 pagini9 Regulation of Blood GlucoseAnand VeerananÎncă nu există evaluări
- Estimation of AlbuminDocument2 paginiEstimation of AlbuminAnand VeerananÎncă nu există evaluări
- Reference ValueDocument2 paginiReference ValueAnand VeerananÎncă nu există evaluări
- 1269Document9 pagini1269Anand VeerananÎncă nu există evaluări
- Cardiac BiomarkersDocument63 paginiCardiac BiomarkersAnand VeerananÎncă nu există evaluări
- Cardiac BiomarkersDocument7 paginiCardiac BiomarkersAnand VeerananÎncă nu există evaluări
- Low Levels of Alkaline Phosphatase in The BloodDocument3 paginiLow Levels of Alkaline Phosphatase in The BloodAnand VeerananÎncă nu există evaluări
- Hormone ActionDocument142 paginiHormone ActionAnand Veeranan100% (1)
- Glucose Tolerance Test Definition: To Assess The Ability of The Body (Pancreas) To Handle A LoadDocument11 paginiGlucose Tolerance Test Definition: To Assess The Ability of The Body (Pancreas) To Handle A LoadAnand VeerananÎncă nu există evaluări
- Fructosse Metabolism For ClassDocument50 paginiFructosse Metabolism For ClassAnand VeerananÎncă nu există evaluări
- Low Levels of Alkaline Phosphatase in The BloodDocument3 paginiLow Levels of Alkaline Phosphatase in The BloodAnand VeerananÎncă nu există evaluări
- Water As A ReagentDocument7 paginiWater As A ReagentAnand VeerananÎncă nu există evaluări
- Biochemical CalculationsDocument458 paginiBiochemical CalculationsAnand VeerananÎncă nu există evaluări
- Mass SpectrometryDocument64 paginiMass SpectrometryAnand VeerananÎncă nu există evaluări
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (120)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Electrolysis ProcessesDocument180 paginiElectrolysis ProcessesEngineering Office Shahrak100% (1)
- Agilent Fat Sol Vit AssayDocument2 paginiAgilent Fat Sol Vit AssaySalafiyyunÎncă nu există evaluări
- yokAcikBilim 10185403Document71 paginiyokAcikBilim 10185403gozdebstnciÎncă nu există evaluări
- Astm f2129Document9 paginiAstm f2129edgmundarayÎncă nu există evaluări
- Heat and Mass Transfer - E. R. G. Eckert and R. M. Drake PDFDocument46 paginiHeat and Mass Transfer - E. R. G. Eckert and R. M. Drake PDFAnaQatarina50% (4)
- Tmecc 0411Document6 paginiTmecc 0411Karen BenteoÎncă nu există evaluări
- Phys 1241Document4 paginiPhys 1241ChrisÎncă nu există evaluări
- TBP, ASTM, and EFV ComparedDocument2 paginiTBP, ASTM, and EFV Comparedvicktorinox230388Încă nu există evaluări
- Numerical Analysis For Energy Performance Optimization of Hollow Bricks For Roofing. Case Study - Hot Climate of AlgeriaDocument10 paginiNumerical Analysis For Energy Performance Optimization of Hollow Bricks For Roofing. Case Study - Hot Climate of Algeriamah0809Încă nu există evaluări
- Chapter 1 - Atoms, Molecules and Stoichiometry PDFDocument10 paginiChapter 1 - Atoms, Molecules and Stoichiometry PDFRamshaÎncă nu există evaluări
- Temperature Control With ThermistorDocument7 paginiTemperature Control With ThermistorMonika Maheshwari100% (1)
- Comparative Evaluation of The Physicochemical and Sensorial Quality of Dragon Fruit Jams Made With Diferent Types of Citrus Juices As Acidulants - Turnitin SubmissionDocument59 paginiComparative Evaluation of The Physicochemical and Sensorial Quality of Dragon Fruit Jams Made With Diferent Types of Citrus Juices As Acidulants - Turnitin SubmissionCheng KaiÎncă nu există evaluări
- Minimum Thermal FlowDocument4 paginiMinimum Thermal Flowdk4monjureÎncă nu există evaluări
- Watford 2001Document7 paginiWatford 2001CARDIO 2019Încă nu există evaluări
- (Alan R. Katritzky, Otto Meth-Cohn, and Charles W.Document1.287 pagini(Alan R. Katritzky, Otto Meth-Cohn, and Charles W.Ganesh KashinathÎncă nu există evaluări
- Role of Micro-OrganismsDocument23 paginiRole of Micro-Organismslinu balanÎncă nu există evaluări
- Prospectus Syllabus: Post Graduate Diploma Course in Food Analysis and Quality AssuranceDocument19 paginiProspectus Syllabus: Post Graduate Diploma Course in Food Analysis and Quality Assurancepriyanka thapliyal100% (1)
- Sop of UV HPLCDocument5 paginiSop of UV HPLCSachin S RaneÎncă nu există evaluări
- Shrimp: In: Use of Sodium Metabisulfite, AlternativesDocument3 paginiShrimp: In: Use of Sodium Metabisulfite, Alternativesvalerie rosalind angkawidjajaÎncă nu există evaluări
- Benjamin. Lewin - GENES V.-Oxford (1994)Document34 paginiBenjamin. Lewin - GENES V.-Oxford (1994)AnkitÎncă nu există evaluări
- CPP & Cqa PDFDocument71 paginiCPP & Cqa PDFanon_695264516100% (1)
- AlkanolamideDocument5 paginiAlkanolamidebellesuperÎncă nu există evaluări
- Apiezon AP100 Grease MSDSDocument5 paginiApiezon AP100 Grease MSDSData Sheet SolutionsÎncă nu există evaluări
- USP-NF Atorvastatin CalciumDocument8 paginiUSP-NF Atorvastatin CalciumPhạm Đức LộcÎncă nu există evaluări
- Physics Today: Quantum CriticalityDocument8 paginiPhysics Today: Quantum CriticalityAndré RojasÎncă nu există evaluări
- Stockmann 2016Document12 paginiStockmann 2016Barbara SilvaÎncă nu există evaluări
- Opportunities and Limits of 2k Injection MouldingDocument22 paginiOpportunities and Limits of 2k Injection Mouldingsa_arunkumarÎncă nu există evaluări
- Bomba Neumatica PB 1/4Document16 paginiBomba Neumatica PB 1/4Marco MendozaÎncă nu există evaluări
- Consolidation Theories of Soils: By: Alemayehu Teferra (Prof., Dr.-Ing.)Document33 paginiConsolidation Theories of Soils: By: Alemayehu Teferra (Prof., Dr.-Ing.)ASAMENEWÎncă nu există evaluări
- 1.7 Evaporative Air Cooling EquipmentDocument8 pagini1.7 Evaporative Air Cooling EquipmentRio BananÎncă nu există evaluări