S-ar putea să vă placă și
- Therapy NotesDocument723 paginiTherapy Notesteaknee100% (1)
- SCHOOL NURSE RESOURCE MANUAL Tenth Edition: Tenth Edition: A Guide to PracticeDe la EverandSCHOOL NURSE RESOURCE MANUAL Tenth Edition: Tenth Edition: A Guide to PracticeÎncă nu există evaluări
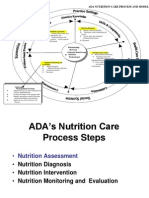
- Nutrition Care Process (NCP)Document48 paginiNutrition Care Process (NCP)annyeong_123100% (1)
- Ortho Bullets Volume One Trauma 2017Document2.548 paginiOrtho Bullets Volume One Trauma 2017Fawzia Haznah Nurul Imani100% (7)
- Nutrition Care Process Briefer CP OrientationDocument37 paginiNutrition Care Process Briefer CP OrientationDadanÎncă nu există evaluări
- Small Animal Clinical Nutrition 5thDocument21 paginiSmall Animal Clinical Nutrition 5thJairo Pereira100% (1)
- Symposium: Challenges in Targeting Nutrition ProgramsDocument5 paginiSymposium: Challenges in Targeting Nutrition ProgramsMukhlidahHanunSiregarÎncă nu există evaluări
- Nutrition Assessment 1Document22 paginiNutrition Assessment 1KHALEEL SALEHÎncă nu există evaluări
- Solution Manual For Nutrition Therapy and Pathophysiology 3rd Edition Nelms Sucher 1305111966 9781305111967Document35 paginiSolution Manual For Nutrition Therapy and Pathophysiology 3rd Edition Nelms Sucher 1305111966 9781305111967mrbrandondavisxrsfzdeimc100% (24)
- "Mode One" Author & Dating Coach Alan Roger Currie Releases Criticism of Alleged Harvey Weinstein BehaviorDocument3 pagini"Mode One" Author & Dating Coach Alan Roger Currie Releases Criticism of Alleged Harvey Weinstein BehaviorPR.com100% (1)
- Nutrition Care ProcessDocument48 paginiNutrition Care ProcessNariÎncă nu există evaluări
- NCPT For EALDocument61 paginiNCPT For EALAsri SubarjatiÎncă nu există evaluări
- Guidelines for Assessing Nutrition-Related Knowledge, Attitudes and PracticesDe la EverandGuidelines for Assessing Nutrition-Related Knowledge, Attitudes and PracticesÎncă nu există evaluări
- AppendicitisDocument14 paginiAppendicitispreethijojo2003558288% (8)
- NCP Eal 201711 PDFDocument64 paginiNCP Eal 201711 PDFAnisaÎncă nu există evaluări
- Process Nutrition Care Terminology (NCPT) : R GHTDocument64 paginiProcess Nutrition Care Terminology (NCPT) : R GHTnoviananurhanifahÎncă nu există evaluări
- History of Philippine LiteratureDocument11 paginiHistory of Philippine LiteratureKyla Ocampo63% (54)
- 4 Strength and Durability of Concrete With LC3Document41 pagini4 Strength and Durability of Concrete With LC3Mirza BasitÎncă nu există evaluări
- Ink Presentation Final (TOYO)Document34 paginiInk Presentation Final (TOYO)komal100% (1)
- Academy Pocket Guide To Pediatric Nutrition 2nd Edition Sample ChapterDocument6 paginiAcademy Pocket Guide To Pediatric Nutrition 2nd Edition Sample ChapterGanes Tiara WidhaÎncă nu există evaluări
- A S P E N Clinical Guidelines - Nutrition Support of The Critically Ill ChildDocument56 paginiA S P E N Clinical Guidelines - Nutrition Support of The Critically Ill ChildPaulina Kristiani BangunÎncă nu există evaluări
- Nutrition SurveillanceDocument4 paginiNutrition Surveillancenimila gopiÎncă nu există evaluări
- HND 309 Nutrition SurveillanceDocument6 paginiHND 309 Nutrition Surveillancehafeesadetunji01Încă nu există evaluări
- Assessment of Nutritional SituationDocument24 paginiAssessment of Nutritional SituationMawasumi Ayu Andini0% (1)
- Dietary AssessmentDocument20 paginiDietary AssessmentharviliaÎncă nu există evaluări
- Nutritional SurveillanceDocument59 paginiNutritional Surveillancekalkidan Hassen AbateÎncă nu există evaluări
- Nutrition SurveyDocument25 paginiNutrition SurveyShreya PokharelÎncă nu există evaluări
- SHS 406 Lec-03Document67 paginiSHS 406 Lec-03Shahzad MazharÎncă nu există evaluări
- Nutrition Information SystemDocument7 paginiNutrition Information SystemAbel AgoroÎncă nu există evaluări
- 7-Nutrition-Intervention 9 0Document68 pagini7-Nutrition-Intervention 9 0Bethel100% (1)
- Ilmu GiziDocument3 paginiIlmu GiziLucy Dwi MawarniÎncă nu există evaluări
- Nutritional Surveillance ModuleDocument57 paginiNutritional Surveillance ModuleDwi Ayu Lestari100% (1)
- The Tools of Nutrition AssessmentDocument12 paginiThe Tools of Nutrition AssessmentJaash De Guzman50% (2)
- Guia ESPEN - Tamizaje NutricionalDocument7 paginiGuia ESPEN - Tamizaje NutricionalJudy OlivaÎncă nu există evaluări
- Assessment of The Nutritional Status of The CommunityDocument29 paginiAssessment of The Nutritional Status of The CommunitySarad Chand YadavÎncă nu există evaluări
- NDT Complete Midterm Lecture 3Document88 paginiNDT Complete Midterm Lecture 3nicolediazÎncă nu există evaluări
- Nutritional Risk Screening and Assessment: Clinical MedicineDocument19 paginiNutritional Risk Screening and Assessment: Clinical MedicineRossmery VeraÎncă nu există evaluări
- Nutrition Month 2014 PresentationDocument66 paginiNutrition Month 2014 PresentationRaine del RosarioÎncă nu există evaluări
- Epidemiologi Gizi Dan Asesmen Diet Untuk Pasien Penyakit GinjalDocument29 paginiEpidemiologi Gizi Dan Asesmen Diet Untuk Pasien Penyakit GinjalRaajih Isma'il Al-FaruqiÎncă nu există evaluări
- Food Security, Poverty and Nutrition Policy Analysis: Statistical Methods and ApplicationsDe la EverandFood Security, Poverty and Nutrition Policy Analysis: Statistical Methods and ApplicationsEvaluare: 4 din 5 stele4/5 (1)
- Food Security in Emergency Areas: Sean Steven Puleh Dept. of Public Health Lira UniversityDocument43 paginiFood Security in Emergency Areas: Sean Steven Puleh Dept. of Public Health Lira UniversityAYO NELSONÎncă nu există evaluări
- 1 2-Feedings-In-DisasterDocument48 pagini1 2-Feedings-In-DisasterFlynn NutÎncă nu există evaluări
- J. Nutr.-1994-Thompson-2245s-317sDocument73 paginiJ. Nutr.-1994-Thompson-2245s-317sAlmaÎncă nu există evaluări
- Notes For Pharmacy StudentsDocument25 paginiNotes For Pharmacy StudentsMaህÎncă nu există evaluări
- WFP CDC A Manual Measuring and Interpreting Malnutrition and MortalityDocument222 paginiWFP CDC A Manual Measuring and Interpreting Malnutrition and Mortalitypneumonomicroscopic100% (1)
- NCP 1st and 2nd StepDocument6 paginiNCP 1st and 2nd StepMehwish MughalÎncă nu există evaluări
- Health - : DieteticsDocument3 paginiHealth - : DieteticsApple BananaÎncă nu există evaluări
- Chap1 Introduction To Nutritional AssessmentDocument32 paginiChap1 Introduction To Nutritional AssessmentAbdi Khalaq Ali Hashi100% (1)
- Nutritional Adequacy of The Mediterranean DietDocument22 paginiNutritional Adequacy of The Mediterranean DietEbaa AbdullatifÎncă nu există evaluări
- Protocol - Generic Nutrition SurveyDocument27 paginiProtocol - Generic Nutrition SurveyMr. ProfessorÎncă nu există evaluări
- NCP 1 Na-SnapDocument1 paginăNCP 1 Na-SnapAlvia ArvenaÎncă nu există evaluări
- Session #2 SAS - Nutrition (Lecture)Document7 paginiSession #2 SAS - Nutrition (Lecture)Mariel Gwen RetorcaÎncă nu există evaluări
- Nutritional EpidemiologyDocument3 paginiNutritional Epidemiologylample100% (1)
- Diagram and TablesDocument9 paginiDiagram and TablesPatricia Denise OrquiaÎncă nu există evaluări
- Nutritional Interventions: Meseret Moroda (MPH in Nutrition) Salale University October, 2023Document48 paginiNutritional Interventions: Meseret Moroda (MPH in Nutrition) Salale University October, 2023Edo JeldeÎncă nu există evaluări
- Dietary Assesement Presentation, Community NutritionDocument75 paginiDietary Assesement Presentation, Community NutritionDoreen NÎncă nu există evaluări
- Food JoshDocument5 paginiFood JoshRulani PrinceÎncă nu există evaluări
- Session 14 - Data Presentation, Dis 237Document13 paginiSession 14 - Data Presentation, Dis 237Lealyn MaquinianoÎncă nu există evaluări
- Nutrition Assesment OverviewDocument5 paginiNutrition Assesment OverviewDea MustikaÎncă nu există evaluări
- Community NutritionDocument35 paginiCommunity NutritionnkhomaslaterÎncă nu există evaluări
- MULTI-SECTORAL NUTRITION STRATEGY 2014-2025 Technical Guidance BriefDocument14 paginiMULTI-SECTORAL NUTRITION STRATEGY 2014-2025 Technical Guidance Briefhyperlycan5Încă nu există evaluări
- 30.04.2013-Food RecordsDocument29 pagini30.04.2013-Food RecordsNada NabilahÎncă nu există evaluări
- Thigpen Matt CurriculumDocument12 paginiThigpen Matt Curriculumapi-261193383Încă nu există evaluări
- Child, Malnutrition Part 1 2023Document23 paginiChild, Malnutrition Part 1 2023www.udarachathuranga20Încă nu există evaluări
- Nutrition Care ProcessDocument44 paginiNutrition Care ProcessKATH GOÎncă nu există evaluări
- Diagnostic Imaging MethodsDocument90 paginiDiagnostic Imaging MethodsKyla OcampoÎncă nu există evaluări
- What Is ?: Ready ToDocument1 paginăWhat Is ?: Ready ToerielleÎncă nu există evaluări
- Cooking VocabularyDocument4 paginiCooking VocabularyKyla OcampoÎncă nu există evaluări
- Journal of Gastroenterology and HepatologyDocument9 paginiJournal of Gastroenterology and HepatologyKyla OcampoÎncă nu există evaluări
- Cell Physiology Part 1Document4 paginiCell Physiology Part 1Kyla OcampoÎncă nu există evaluări
- Aliquam Venenatis Nunc at Enim.: Lorem Ipsum Dolor Sit AmetDocument5 paginiAliquam Venenatis Nunc at Enim.: Lorem Ipsum Dolor Sit AmetKyla OcampoÎncă nu există evaluări
- Laws and LegislationsDocument3 paginiLaws and LegislationsKyla OcampoÎncă nu există evaluări
- Public Health NutritionistDocument3 paginiPublic Health NutritionistKyla OcampoÎncă nu există evaluări
- Nutrition Program: Common Nutritional Deficiencies 1. Vitamin A 2. Iron 3. IodineDocument26 paginiNutrition Program: Common Nutritional Deficiencies 1. Vitamin A 2. Iron 3. IodineKyla OcampoÎncă nu există evaluări
- Business Letter 3 PDFDocument1 paginăBusiness Letter 3 PDFKyla OcampoÎncă nu există evaluări
- Christian Living Education IVDocument2 paginiChristian Living Education IVKyla OcampoÎncă nu există evaluări
- Protein Lab ReportDocument22 paginiProtein Lab ReportKyla OcampoÎncă nu există evaluări
- BiologyDocument3 paginiBiologyKyla OcampoÎncă nu există evaluări
- Tolerance Chart: (Maximum Permissible Error)Document3 paginiTolerance Chart: (Maximum Permissible Error)arif_setyaw4nÎncă nu există evaluări
- Pay & PADocument5 paginiPay & PApujiptÎncă nu există evaluări
- Time ManagementDocument1 paginăTime ManagementZaidi1Încă nu există evaluări
- Digital Meter: KIT No: 0349 307 620Document6 paginiDigital Meter: KIT No: 0349 307 620Garlin MunarÎncă nu există evaluări
- Early Theories On The Origin of Life On Earth: Creation TheoryDocument1 paginăEarly Theories On The Origin of Life On Earth: Creation TheoryAngel Elizaga IIÎncă nu există evaluări
- Sandwich StoichiometryDocument2 paginiSandwich StoichiometryMaysaa El HarakehÎncă nu există evaluări
- 327 - Mil-C-15074Document2 pagini327 - Mil-C-15074Bianca MoraisÎncă nu există evaluări
- Components of FitnessDocument3 paginiComponents of Fitnessapi-3830277100% (1)
- The Safe Motherhood InitiativeDocument3 paginiThe Safe Motherhood InitiativeAnonymous g6L7jJWÎncă nu există evaluări
- 1 s2.0 S0378517311000226 MainDocument9 pagini1 s2.0 S0378517311000226 MainFIRMAN MUHARAMÎncă nu există evaluări
- 1-1FlowCharts For HaccpDocument3 pagini1-1FlowCharts For HaccpPeter George0% (1)
- Electron Configurations of The Elements (Data Page) - WikipediaDocument25 paginiElectron Configurations of The Elements (Data Page) - WikipediaAlex OmungaÎncă nu există evaluări
- Tinda Tomato PachadiDocument1 paginăTinda Tomato PachadijyosriÎncă nu există evaluări
- Material Science & Metallurgy: Third Semester B.E. Degree (CBCS) Examination, Dec.2016/Jan.2017Document2 paginiMaterial Science & Metallurgy: Third Semester B.E. Degree (CBCS) Examination, Dec.2016/Jan.2017Shaikh MuzaffarÎncă nu există evaluări
- Pizza Hut and Dominos - A Comparative AnalysisDocument19 paginiPizza Hut and Dominos - A Comparative AnalysisSarvesh Kumar GautamÎncă nu există evaluări
- Fdocuments - in From The Margins To The Mainstream Disaster Research at The CrossroadsDocument26 paginiFdocuments - in From The Margins To The Mainstream Disaster Research at The CrossroadsHanan M. HadidiÎncă nu există evaluări
- 4th Laboratory Activity Gallus DomesticusDocument4 pagini4th Laboratory Activity Gallus DomesticusZia Ammarah SaripÎncă nu există evaluări
- Minibeasts Differentiated Reading Comprehension ActivityDocument15 paginiMinibeasts Differentiated Reading Comprehension Activitymariam helmyÎncă nu există evaluări
- Cell Reproduction Practice ExamDocument5 paginiCell Reproduction Practice Examjacky qianÎncă nu există evaluări
- LOKRING Technical Documentation Submittal Brass enDocument32 paginiLOKRING Technical Documentation Submittal Brass enYamilelcÎncă nu există evaluări
- 2019 MAPEH Baler - Grade 6Document6 pagini2019 MAPEH Baler - Grade 6Maria Rosario VelicariaÎncă nu există evaluări
- Hindustan Coca-Cola Beverages PVT LTD B-91 Mayapuri Industrial Area Phase-I New DelhiDocument2 paginiHindustan Coca-Cola Beverages PVT LTD B-91 Mayapuri Industrial Area Phase-I New DelhiUtkarsh KadamÎncă nu există evaluări
- Uas Semt Genap Fix BING XIDocument12 paginiUas Semt Genap Fix BING XISaepulloh KurniaÎncă nu există evaluări
- Transmission Line BOQ VIMPDocument72 paginiTransmission Line BOQ VIMPkajale_shrikant2325Încă nu există evaluări
- Material Safety Data Sheet Glyphosate 5.4Document5 paginiMaterial Safety Data Sheet Glyphosate 5.4Ahfi Rizqi FajrinÎncă nu există evaluări
- MR Afnan CVDocument3 paginiMR Afnan CVShazada Dauod Khan100% (1)