S-ar putea să vă placă și
- Atelectasis, (Lung Collapse) A Simple Guide To The Condition, Diagnosis, Treatment And Related DiseasesDe la EverandAtelectasis, (Lung Collapse) A Simple Guide To The Condition, Diagnosis, Treatment And Related DiseasesÎncă nu există evaluări
- Cor Pulmonale: Dr. Gerrard UyDocument13 paginiCor Pulmonale: Dr. Gerrard Uyfaridah azzah sariÎncă nu există evaluări
- Valvular Heart DiseaseDocument42 paginiValvular Heart DiseaseareeparambilÎncă nu există evaluări
- Pleural Effusion, A Simple Guide To The Condition, Treatment And Related ConditionsDe la EverandPleural Effusion, A Simple Guide To The Condition, Treatment And Related ConditionsÎncă nu există evaluări
- Myocardial InfarctionDocument18 paginiMyocardial Infarctionporing500Încă nu există evaluări
- 10 CardiomyopathyDocument71 pagini10 CardiomyopathyAnonymous vUEDx8100% (5)
- Hypovolemic Shock: Dr. Sherwin BuluranDocument8 paginiHypovolemic Shock: Dr. Sherwin BuluranChristian UretaÎncă nu există evaluări
- How To Write Killer AdsDocument15 paginiHow To Write Killer Adshfi11939100% (9)
- Cardiac TamponadeDocument10 paginiCardiac TamponadeRahmi Fatma SariÎncă nu există evaluări
- Deep Vein ThrombosisDocument42 paginiDeep Vein ThrombosisNsklm100% (7)
- CardiomyopathyDocument18 paginiCardiomyopathyDimpal Choudhary100% (1)
- Pulmonary Edema: (Acute Heart Failure)Document7 paginiPulmonary Edema: (Acute Heart Failure)james garcia100% (5)
- Rheumatic Heart DiseaseDocument25 paginiRheumatic Heart DiseaseMag5Încă nu există evaluări
- Arrythmia Review TableDocument6 paginiArrythmia Review TablealobrienÎncă nu există evaluări
- Pulmonary EmbolismDocument54 paginiPulmonary Embolismعزيزي أحمد نوردين0% (1)
- Congestive Heart FailureDocument43 paginiCongestive Heart FailuresudersonÎncă nu există evaluări
- Aortic Regurgitation (Ar)Document18 paginiAortic Regurgitation (Ar)rameshbmc100% (1)
- P EmbolismDocument29 paginiP EmbolismCommandoCitotz100% (1)
- Pulmonaryembolism 150329161109 Conversion Gate01Document60 paginiPulmonaryembolism 150329161109 Conversion Gate01Rafika RaraÎncă nu există evaluări
- Infective Endocarditis: Christine Joy F. Baquiran MED-3CDocument46 paginiInfective Endocarditis: Christine Joy F. Baquiran MED-3CAbigail SabinoÎncă nu există evaluări
- Etiology and Pathophysiology of Pleural EffusionDocument17 paginiEtiology and Pathophysiology of Pleural EffusionFelix Wafula MusibiÎncă nu există evaluări
- Drug Book On EmergencyDocument21 paginiDrug Book On EmergencyDimpal Choudhary100% (4)
- Occt651 - Occupational Profile Paper - FinalDocument20 paginiOcct651 - Occupational Profile Paper - Finalapi-293182319Încă nu există evaluări
- ENT MCQS (Ear, Pharynx, Tonsils, Deep Neck Infections, Oral Cavity)Document88 paginiENT MCQS (Ear, Pharynx, Tonsils, Deep Neck Infections, Oral Cavity)sidsudp75% (4)
- Quizbee 2019 Nutrition Month EasyDocument4 paginiQuizbee 2019 Nutrition Month EasyJaenicaPaulineCristobalÎncă nu există evaluări
- Pulmonary EmbolismDocument21 paginiPulmonary EmbolismMadhu Bala100% (2)
- PneumothoraxDocument52 paginiPneumothoraxtrisna satrianaÎncă nu există evaluări
- Mitral StenosisDocument43 paginiMitral StenosisEricka SantosÎncă nu există evaluări
- Valvular Heart DiseaseDocument54 paginiValvular Heart DiseaseRommanah AzmiÎncă nu există evaluări
- Mitral Stenosis Mitral RegurgitationDocument66 paginiMitral Stenosis Mitral RegurgitationMarshellaTriPradilagaÎncă nu există evaluări
- Mechanical VentilationDocument19 paginiMechanical VentilationDoha EbedÎncă nu există evaluări
- Pulmonary EdemaDocument10 paginiPulmonary EdemaNader Smadi100% (6)
- BRONCHIECTASISDocument18 paginiBRONCHIECTASISHariz Thaha100% (1)
- Respiratory AcidosisDocument16 paginiRespiratory AcidosisIssa GutierrezÎncă nu există evaluări
- Heart Muscle Shortness of Breath Tired Swelling of The Legs Heart Failure Irregular Heart Beat Fainting Sudden Cardiac DeathDocument6 paginiHeart Muscle Shortness of Breath Tired Swelling of The Legs Heart Failure Irregular Heart Beat Fainting Sudden Cardiac DeathSachin DwivediÎncă nu există evaluări
- Pulmonary EmbolismDocument96 paginiPulmonary Embolismsamice5100% (1)
- Valvular Heart DiseaseDocument73 paginiValvular Heart Diseaseindia2puppy100% (4)
- CopdDocument51 paginiCopdFretzie Anne Gonzales Gomez100% (2)
- Heart BlockDocument10 paginiHeart BlockEköw Santiago JavierÎncă nu există evaluări
- Mitral RegurgitationDocument43 paginiMitral Regurgitationraissasafitry100% (1)
- CopdDocument60 paginiCopdRizqy Shofianingrum100% (1)
- Acute Respiratory FailureDocument17 paginiAcute Respiratory FailurejulianajosÎncă nu există evaluări
- Pulmonary EmbolismDocument23 paginiPulmonary EmbolismBianca Dizon0% (1)
- 13.acute Respiratory FailureDocument34 pagini13.acute Respiratory Failurekarim hassan100% (1)
- Pulmonary EmbolismDocument46 paginiPulmonary EmbolismAnusha VergheseÎncă nu există evaluări
- Empyema: By-Komal JaiswalDocument29 paginiEmpyema: By-Komal JaiswalOlga GoryachevaÎncă nu există evaluări
- Pulmonary EmbolismDocument16 paginiPulmonary EmbolismEhab Mokhtar WehebaÎncă nu există evaluări
- Hodgkin LymphomaDocument32 paginiHodgkin LymphomaAndi SusiloÎncă nu există evaluări
- Chronic Kidney DiseaseDocument49 paginiChronic Kidney Diseasesarguss1471% (7)
- CHF PathophysiologyDocument12 paginiCHF PathophysiologyprofgambhirÎncă nu există evaluări
- Pleural EffusionDocument54 paginiPleural EffusionNovi KurnasariÎncă nu există evaluări
- BRONCHIECTASISDocument36 paginiBRONCHIECTASISNishanth ReddyÎncă nu există evaluări
- 2020 Diagnosiscodefrequencies AsDocument710 pagini2020 Diagnosiscodefrequencies AsM del100% (1)
- Lung Abscess PDFDocument57 paginiLung Abscess PDFRibhav GuptaÎncă nu există evaluări
- Pulmonary EmbolismDocument80 paginiPulmonary EmbolismVarun B Renukappa100% (1)
- Tetralogy of Fallot TofDocument37 paginiTetralogy of Fallot TofWiza ErlandaÎncă nu există evaluări
- Pulmonary EmbolismDocument14 paginiPulmonary EmbolismAngel Naypes ReyesÎncă nu există evaluări
- Constrictive PericarditisDocument54 paginiConstrictive PericarditisRazib AlamÎncă nu există evaluări
- Pathophysiology of MalariaDocument20 paginiPathophysiology of Malariamelia100% (1)
- Cardiogenic Shock: BY Dr. M L Patel MD Associate Professor Deptt. of MedicineDocument19 paginiCardiogenic Shock: BY Dr. M L Patel MD Associate Professor Deptt. of MedicineDurgesh PushkarÎncă nu există evaluări
- Heart Failure With Preserved Ejection FractionDocument19 paginiHeart Failure With Preserved Ejection Fractioncosmin balanÎncă nu există evaluări
- Mitral Stenosis, NicvdDocument33 paginiMitral Stenosis, NicvdNavojit ChowdhuryÎncă nu există evaluări
- ArdsDocument81 paginiArdsAmit KlÎncă nu există evaluări
- Pulmonary EmbolismDocument47 paginiPulmonary EmbolismmalathiÎncă nu există evaluări
- Pulmonary Embolus (PE)Document3 paginiPulmonary Embolus (PE)Heidi M FischerÎncă nu există evaluări
- Deep Venous Thrombosis and Pulmonary ThromboembolismDocument19 paginiDeep Venous Thrombosis and Pulmonary ThromboembolismTaqdees ManzoorÎncă nu există evaluări
- DVT Pulmonary EmbolismDocument40 paginiDVT Pulmonary EmbolismDr. Shatdal ChaudharyÎncă nu există evaluări
- A Case of Alport Syndrome Presented With Bilateral Anterior LenticonusDocument3 paginiA Case of Alport Syndrome Presented With Bilateral Anterior LenticonusBOHR International Journal of Current Research in Optometry and Ophthalmology (BIJCROO)Încă nu există evaluări
- Respiratory System Assessment PDFDocument53 paginiRespiratory System Assessment PDFJay RomeÎncă nu există evaluări
- RBCs Abnormal Morphology FinalDocument33 paginiRBCs Abnormal Morphology FinalInahkoni Alpheus Sky OiragasÎncă nu există evaluări
- PregnancyDocument11 paginiPregnancyLyra IsraelÎncă nu există evaluări
- Eye & ENTDocument12 paginiEye & ENTShandar SadafÎncă nu există evaluări
- Classification: Indication: CNS: Ototoxicity-: Name: L.Y.C Age/Sex: 59 Y.o/ FDocument8 paginiClassification: Indication: CNS: Ototoxicity-: Name: L.Y.C Age/Sex: 59 Y.o/ FEden Marie FranciscoÎncă nu există evaluări
- Cardiovascular Review PDFDocument6 paginiCardiovascular Review PDFMacy Grace Yuzon GuingabÎncă nu există evaluări
- Inflammation Digestive Tract Ileum Small Intestine Stomach: Crohn Disease Regional Enteritis Regional IleitisDocument10 paginiInflammation Digestive Tract Ileum Small Intestine Stomach: Crohn Disease Regional Enteritis Regional IleitisOlivia BakerÎncă nu există evaluări
- PONSTAN® Capsules: What Is in This LeafletDocument4 paginiPONSTAN® Capsules: What Is in This LeafletLee Hye RiÎncă nu există evaluări
- Jurnal Virgin Coconut Oil (VCO)Document8 paginiJurnal Virgin Coconut Oil (VCO)Tamam Ibrahim SatrioÎncă nu există evaluări
- Budd-Chiari Syndrome: Spectrum of Imaging FindingsDocument9 paginiBudd-Chiari Syndrome: Spectrum of Imaging FindingsDanaAmaranducaiÎncă nu există evaluări
- K25 - A - Congenital Anomalies of The Urinary TractDocument26 paginiK25 - A - Congenital Anomalies of The Urinary TractErwin SiregarÎncă nu există evaluări
- Propeduetic Pediatrics Class 1Document11 paginiPropeduetic Pediatrics Class 1RockybhaiÎncă nu există evaluări
- Hepatitis B in PregnancyDocument46 paginiHepatitis B in Pregnancycitra dewiÎncă nu există evaluări
- Kulit Emergency in DermatologyDocument47 paginiKulit Emergency in DermatologyAulia Shabrina SyukharialÎncă nu există evaluări
- Drug Study: SaluronDocument4 paginiDrug Study: Saluronunkown userÎncă nu există evaluări
- First Step To Achieve Your ObjectiveDocument7 paginiFirst Step To Achieve Your ObjectiveNicole Ivy GorimoÎncă nu există evaluări
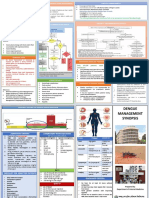
- Dengue Management Synopsis BSMMUDocument2 paginiDengue Management Synopsis BSMMURakibk65Încă nu există evaluări
- Syringomyelia, Arachnoiditis and SpasticityDocument53 paginiSyringomyelia, Arachnoiditis and SpasticitySam OlukaÎncă nu există evaluări
- ExamView - Chapter - 05Document6 paginiExamView - Chapter - 05Stella WangÎncă nu există evaluări
- Therapy in TuberculosisDocument4 paginiTherapy in TuberculosisSamir SkejicÎncă nu există evaluări
- UNIVERSITY of SAN AGUSTIN - Capillary Electrophoresis Lecture 2023Document231 paginiUNIVERSITY of SAN AGUSTIN - Capillary Electrophoresis Lecture 2023alyssa apudÎncă nu există evaluări
- Hypokalemic Paralysis PDFDocument7 paginiHypokalemic Paralysis PDFFanny SimaÎncă nu există evaluări