S-ar putea să vă placă și
- د.عبد الزهره THE GYNAECOLOGICAL EXAMINATION-1 (Muhadharaty)Document29 paginiد.عبد الزهره THE GYNAECOLOGICAL EXAMINATION-1 (Muhadharaty)MohammedÎncă nu există evaluări
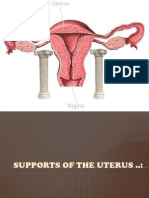
- Supports of The UterusDocument20 paginiSupports of The UterusAshwin Prem Solomon100% (1)
- Menstrual Disorders: Olufemi Aworinde Lecturer/ Consultant Obstetrician and Gynaecologist, Bowen University, IwoDocument36 paginiMenstrual Disorders: Olufemi Aworinde Lecturer/ Consultant Obstetrician and Gynaecologist, Bowen University, IwoAkinbani MoyosoreÎncă nu există evaluări
- POP June 10,2021 1Document48 paginiPOP June 10,2021 1Kerod AbebeÎncă nu există evaluări
- Chronic Pelvic Pain2010Document48 paginiChronic Pelvic Pain2010Feruza SultanmuratovaÎncă nu există evaluări
- C SectionDocument50 paginiC SectionAlano S. LimgasÎncă nu există evaluări
- Pop QDocument45 paginiPop QObgyn Maret2016Încă nu există evaluări
- Bartholin's Cyst/AbscessDocument6 paginiBartholin's Cyst/AbscessJane NathaniaÎncă nu există evaluări
- Mullarian AnomoliesDocument85 paginiMullarian AnomoliesPrathibha GuruguriÎncă nu există evaluări
- Laparoscopic Gynecologist Surgeon in HSR Layout BangaloreDocument8 paginiLaparoscopic Gynecologist Surgeon in HSR Layout BangaloreDr.Beena JeysinghÎncă nu există evaluări
- PA Genitalia WanitaDocument100 paginiPA Genitalia WanitaBÎncă nu există evaluări
- Neonatal Intestinal Obstruction EPSGHAN PDFDocument77 paginiNeonatal Intestinal Obstruction EPSGHAN PDFRobert ChristevenÎncă nu există evaluări
- (New) Early Pregnancy Complications RDocument51 pagini(New) Early Pregnancy Complications RMesk Banat100% (2)
- Pop, RevDocument139 paginiPop, RevYusof AndreiÎncă nu există evaluări
- Hysteroscopic Limitations PDFDocument59 paginiHysteroscopic Limitations PDFV R100% (1)
- Gynecological History Taking and ExaminationDocument17 paginiGynecological History Taking and Examinationnmsiswaridewi100% (1)
- Blood Supply Pelvic OrgansDocument39 paginiBlood Supply Pelvic OrgansoliviaÎncă nu există evaluări
- Obs History Taking FormatDocument24 paginiObs History Taking FormatBibek PandeyÎncă nu există evaluări
- Difficulties in Vaginal HysterctomyDocument66 paginiDifficulties in Vaginal HysterctomyManamita NiphadkarÎncă nu există evaluări
- Adnexal Torsion: Maria Giroux, HBSC, MDDocument33 paginiAdnexal Torsion: Maria Giroux, HBSC, MDMistiru TegegneÎncă nu există evaluări
- Acog Practice Bulletin Summary: Pregestational Diabetes MellitusDocument3 paginiAcog Practice Bulletin Summary: Pregestational Diabetes MellitusMaría Fernanda Palma AcostaÎncă nu există evaluări
- Carcinoma Penis Management: Dr. Lilamani Rajthala MS Resident Moderator: Dr. Samir ShresthaDocument63 paginiCarcinoma Penis Management: Dr. Lilamani Rajthala MS Resident Moderator: Dr. Samir ShresthaBibek GhimireÎncă nu există evaluări
- Genital FistulaeDocument15 paginiGenital Fistulaesangeetha francisÎncă nu există evaluări
- Early Pregnancy Problems: Presented byDocument28 paginiEarly Pregnancy Problems: Presented byMalk OmryÎncă nu există evaluări
- 8surgical Management of Dysfunctional Uterine Bleeding - KabilanDocument14 pagini8surgical Management of Dysfunctional Uterine Bleeding - KabilanNavani TharanÎncă nu există evaluări
- Obstetrics and Gynecological InstrumentsDocument31 paginiObstetrics and Gynecological InstrumentsGAYATHRI RAKESHÎncă nu există evaluări
- BreastDocument49 paginiBreastcryphonexyÎncă nu există evaluări
- Infertility IDocument36 paginiInfertility Idr_asaleh100% (1)
- Operative GynaecologyDocument59 paginiOperative GynaecologyArun Shree R0% (1)
- Clinical Practice Guideline For The Management of Anorectal Abscess Fistula-In-Ano and Rectovaginal FistulaDocument17 paginiClinical Practice Guideline For The Management of Anorectal Abscess Fistula-In-Ano and Rectovaginal FistulaAlivia HanumÎncă nu există evaluări
- Obstetric Anal Sphincter Injury (OASIS) - UpToDateDocument39 paginiObstetric Anal Sphincter Injury (OASIS) - UpToDateErickÎncă nu există evaluări
- Anal Fissure: BY Alisha SaleemDocument7 paginiAnal Fissure: BY Alisha Saleemashar khanÎncă nu există evaluări
- Non-Surgical and Surgical Management of Pelvic OrgDocument10 paginiNon-Surgical and Surgical Management of Pelvic OrgAhmed AnwarÎncă nu există evaluări
- CarcinomaofbreastDocument71 paginiCarcinomaofbreastAghisha Subeesh100% (1)
- Llewellyn-Jones Fundamentals of Obstetrics and Gynecology Part-5Document42 paginiLlewellyn-Jones Fundamentals of Obstetrics and Gynecology Part-5Baraa M. Nouri KharbotliÎncă nu există evaluări
- The Ten-Step Vaginal Hysterectomy - A Newer and Better ApproachDocument8 paginiThe Ten-Step Vaginal Hysterectomy - A Newer and Better ApproachqisthiaufaÎncă nu există evaluări
- Presented by DR - Shahbaz Ahmad Professor of Community MedicineDocument76 paginiPresented by DR - Shahbaz Ahmad Professor of Community MedicinePriya bhattiÎncă nu există evaluări
- Abortion PresentationDocument46 paginiAbortion PresentationJhong Xyrus67% (3)
- The Management of Asherman Syndrome: A Review of LiteratureDocument11 paginiThe Management of Asherman Syndrome: A Review of LiteratureEuphra Adellheid100% (1)
- Principles of Safe LaparosDocument28 paginiPrinciples of Safe Laparosolyviutza16Încă nu există evaluări
- Case Presentation Testicular TorsonDocument16 paginiCase Presentation Testicular TorsonMestikarini AstariÎncă nu există evaluări
- Obstetric Gynaecology Jan 11Document32 paginiObstetric Gynaecology Jan 11selvie87Încă nu există evaluări
- Genital FistulaeDocument27 paginiGenital Fistulaeapi-3705046100% (1)
- Total Pelvic ExenterationDocument13 paginiTotal Pelvic ExenterationRirin Wahyuni100% (1)
- UTI On A Background of Obstructive NephropathyDocument26 paginiUTI On A Background of Obstructive NephropathyAminath MeesanÎncă nu există evaluări
- AMTSL BrieferDocument2 paginiAMTSL BrieferNewborn2013Încă nu există evaluări
- Tuberculosis in Obstetrics and GynecologyDocument42 paginiTuberculosis in Obstetrics and GynecologyameenÎncă nu există evaluări
- Menstrual AbnormalitiesDocument77 paginiMenstrual AbnormalitiesAlivia SoerayaÎncă nu există evaluări
- Uterine FibroidsDocument21 paginiUterine FibroidsPrasun BiswasÎncă nu există evaluări
- ALARMER Dystocia PDFDocument5 paginiALARMER Dystocia PDFwilliamÎncă nu există evaluări
- TOG Vaginal HysterectomyDocument6 paginiTOG Vaginal HysterectomyYasmin AlkhatibÎncă nu există evaluări
- WP GynaeExams4Document37 paginiWP GynaeExams4Ahsan JamÎncă nu există evaluări
- 2015 Oncology CREOG Review PDFDocument76 pagini2015 Oncology CREOG Review PDFRima HajjarÎncă nu există evaluări
- Acute Urinary RetentionDocument26 paginiAcute Urinary Retentionlukmankyubi100% (1)
- Urinary IncontinenceDocument16 paginiUrinary IncontinenceOana BalintÎncă nu există evaluări
- Vesicovaginal FistulaDocument7 paginiVesicovaginal Fistuladrnareshkumar3281Încă nu există evaluări
- Omphalocele & Gastroschisis - SNguyenDocument21 paginiOmphalocele & Gastroschisis - SNguyenherdigunantaÎncă nu există evaluări
- Hernia: Inguinal - Surgical Anatomy, Presentation, Treatment, ComplicationsDocument43 paginiHernia: Inguinal - Surgical Anatomy, Presentation, Treatment, ComplicationsFobin VargheseÎncă nu există evaluări
- Mohsen AttiaDocument3 paginiMohsen AttiaAloah122346100% (1)
- Birthstones of All MonthsDocument15 paginiBirthstones of All MonthssmbawasainiÎncă nu există evaluări
- Medical Ethics/ 5 QuestionsDocument2 paginiMedical Ethics/ 5 QuestionssmbawasainiÎncă nu există evaluări
- MCCEE Questions For IMGsDocument30 paginiMCCEE Questions For IMGssmbawasainiÎncă nu există evaluări
- ACLS Supplementary Material PDFDocument74 paginiACLS Supplementary Material PDFsmbawasainiÎncă nu există evaluări
- A Hundred Questions in ObstetricsDocument30 paginiA Hundred Questions in ObstetricssmbawasainiÎncă nu există evaluări
- Infant IntroDocument86 paginiInfant IntrosmbawasainiÎncă nu există evaluări
- Kahn IntlSocietyDiseaseSurvConf 12-3-09Document51 paginiKahn IntlSocietyDiseaseSurvConf 12-3-09smbawasainiÎncă nu există evaluări
- Answer: B... and The First Case Came To The Attention of The Investigator Is Called Index CaseDocument6 paginiAnswer: B... and The First Case Came To The Attention of The Investigator Is Called Index Casesmbawasaini0% (1)
- 5th Lecture - Prevention & Control of Diseases - 12 Dec 2015Document41 pagini5th Lecture - Prevention & Control of Diseases - 12 Dec 2015smbawasainiÎncă nu există evaluări
- Rapid Sand Filtration - 120227Document20 paginiRapid Sand Filtration - 120227smbawasainiÎncă nu există evaluări
- Guidance Tool For TB Notification in India - FINALDocument92 paginiGuidance Tool For TB Notification in India - FINALYogendra UikeyÎncă nu există evaluări
- Skin MCQ Wo AnsDocument2 paginiSkin MCQ Wo Anssmbawasaini100% (1)
- Total PopulationDocument1 paginăTotal PopulationsmbawasainiÎncă nu există evaluări
- Month OPD IPD: January February March April May June July August September October November DecemberDocument3 paginiMonth OPD IPD: January February March April May June July August September October November DecembersmbawasainiÎncă nu există evaluări
- Epidemiological Exercises..Document16 paginiEpidemiological Exercises..smbawasaini100% (1)
- Patient Notification FormatDocument1 paginăPatient Notification FormatsmbawasainiÎncă nu există evaluări
- IMNCI Training Module 1-9Document356 paginiIMNCI Training Module 1-9smbawasaini50% (4)
- MCQ Companion To Applied Radiological Anatomy - MyDocument213 paginiMCQ Companion To Applied Radiological Anatomy - MySharifa AbdulghaffarÎncă nu există evaluări
- AlopeciaDocument90 paginiAlopeciasmbawasainiÎncă nu există evaluări
- Spiritual Health RevisedDocument50 paginiSpiritual Health RevisedsmbawasainiÎncă nu există evaluări
- Ngo & PPDocument38 paginiNgo & PPsmbawasaini100% (1)
- Module 1 To 4Document208 paginiModule 1 To 4smbawasainiÎncă nu există evaluări
- Guidelines For PMDT in India - May 2012Document199 paginiGuidelines For PMDT in India - May 2012smbawasainiÎncă nu există evaluări
- UTS Learning ModuleDocument27 paginiUTS Learning ModuleMichelle ErmacÎncă nu există evaluări
- Case PresentationDocument64 paginiCase PresentationOlivelhynn Bernaldo100% (1)
- Prevalence of Vaginal Candidiasis in Pregnancy Among Coastal South Indian Women HnYuDocument3 paginiPrevalence of Vaginal Candidiasis in Pregnancy Among Coastal South Indian Women HnYuEdogawa RakhmanÎncă nu există evaluări
- Presentation Somatic Sexology Marlene de Beer Ssw1Document12 paginiPresentation Somatic Sexology Marlene de Beer Ssw1sudhakara.rr359Încă nu există evaluări
- Aquifer Case - Summary - FamilyMedicine17 - 55-YDocument9 paginiAquifer Case - Summary - FamilyMedicine17 - 55-YHyunsoo EllisÎncă nu există evaluări
- Give Woman A Hand JobDocument3 paginiGive Woman A Hand JobSparky100% (6)
- Pedia GyneDocument13 paginiPedia Gynerjh1895Încă nu există evaluări
- Mop Bu o Loiu Bert SeazDocument22 paginiMop Bu o Loiu Bert Seazbill5Încă nu există evaluări
- P ('t':'3', 'I':'3053926525') D '' Var B Location Settimeout (Function ( If (Typeof Window - Iframe 'Undefined') ( B.href B.href ) ), 15000)Document14 paginiP ('t':'3', 'I':'3053926525') D '' Var B Location Settimeout (Function ( If (Typeof Window - Iframe 'Undefined') ( B.href B.href ) ), 15000)Ni Wayan Ana PsÎncă nu există evaluări
- Patient Profile-C in The WDocument17 paginiPatient Profile-C in The WPj TignimanÎncă nu există evaluări
- TuberkulozaDocument2 paginiTuberkulozaDen HelfyÎncă nu există evaluări
- Mcqs For Mrcog Part 1 - Richard de CourcyDocument118 paginiMcqs For Mrcog Part 1 - Richard de Courcyprincessmeleana6499Încă nu există evaluări
- Combination of Pelvic Floor and Abdominal Muscle eDocument5 paginiCombination of Pelvic Floor and Abdominal Muscle eNeha SinghÎncă nu există evaluări
- Fertility InnDocument15 paginiFertility Innkunnamon1234100% (2)
- Female Reproductive System UpdatedDocument84 paginiFemale Reproductive System UpdatedAtie IzzatiÎncă nu există evaluări
- 2 Reproductive Tract InfectionsDocument14 pagini2 Reproductive Tract InfectionsawalsherÎncă nu există evaluări
- What Is Low Birth WeightDocument3 paginiWhat Is Low Birth WeightPrincess BartolomeÎncă nu există evaluări
- Chapter 7 (Margot-Desevo)Document10 paginiChapter 7 (Margot-Desevo)Jesse ParkÎncă nu există evaluări
- Passives For V.9a.nDocument141 paginiPassives For V.9a.nMuchairildÎncă nu există evaluări
- Case Study 2ND Yr 1Document21 paginiCase Study 2ND Yr 1Samantha BolanteÎncă nu există evaluări
- Abdomen - Pelvis: Lecturer: Prof. Dr. Wahyuni Lukita Atmodjo, PH.DDocument33 paginiAbdomen - Pelvis: Lecturer: Prof. Dr. Wahyuni Lukita Atmodjo, PH.DAgatha FeliciaÎncă nu există evaluări
- Idoc - Pub - e Book KunyazaDocument27 paginiIdoc - Pub - e Book KunyazaAkorli50% (2)
- WHO FGM GuidelinesDocument64 paginiWHO FGM GuidelinesMuhammmed abdi wahaabÎncă nu există evaluări
- The Role of Physical Therapy in Sexual Health in Men and WomenDocument11 paginiThe Role of Physical Therapy in Sexual Health in Men and WomenJorgeGalleguillosCavadaÎncă nu există evaluări
- Wild Woman in The Bedroom EbookDocument56 paginiWild Woman in The Bedroom EbookredleberaÎncă nu există evaluări
- CatheterizationDocument3 paginiCatheterizationLawrence Cada NofiesÎncă nu există evaluări
- 11 Obstetrics Gynaecology 1Document54 pagini11 Obstetrics Gynaecology 1mobashwer ahmedÎncă nu există evaluări
- Sexual TerminologyDocument2 paginiSexual TerminologyPam BelkevitzÎncă nu există evaluări
- Uterovaginal ProlapseDocument52 paginiUterovaginal ProlapseAmeera K Khan75% (4)
- 208-230 CH08 Lowdermilk - QXDDocument23 pagini208-230 CH08 Lowdermilk - QXDSyarifah Ro'fahÎncă nu există evaluări