S-ar putea să vă placă și
- Diabetic Nephropathy, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDe la EverandDiabetic Nephropathy, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsÎncă nu există evaluări
- Heart Failure With Preserved Ejection FractionDocument19 paginiHeart Failure With Preserved Ejection Fractioncosmin balanÎncă nu există evaluări
- Diabetes Mellitus Type 2Document16 paginiDiabetes Mellitus Type 2MTs MIFDAÎncă nu există evaluări
- Interactive Session On Sodium Homeostasis: Dr.M.Emmanuel Bhaskar Assistant Professor in Medicine SRMC & RiDocument64 paginiInteractive Session On Sodium Homeostasis: Dr.M.Emmanuel Bhaskar Assistant Professor in Medicine SRMC & Ridrbhaskar100% (4)
- CKDDocument35 paginiCKDgailÎncă nu există evaluări
- Acute Renal Failure: Dr. Bobi Ahmad S, S.KPDocument62 paginiAcute Renal Failure: Dr. Bobi Ahmad S, S.KPdr.Bobi Ahmad Sahid, S.KepÎncă nu există evaluări
- Diabetic NephropathyDocument6 paginiDiabetic NephropathyZulfadliZulfadliÎncă nu există evaluări
- Case Study For Chronic Renal FailureDocument6 paginiCase Study For Chronic Renal FailureGabbii CincoÎncă nu există evaluări
- Esrd FinalDocument26 paginiEsrd FinalCreighton A. BayonganÎncă nu există evaluări
- Intro-ESRD Case StudyDocument2 paginiIntro-ESRD Case StudyAngel SamonteÎncă nu există evaluări
- CKD PresentationDocument51 paginiCKD PresentationBasneyatPragyanÎncă nu există evaluări
- Ped Nephro 3rd Ed SchaeferDocument10 paginiPed Nephro 3rd Ed SchaeferAlonso Rodriguez EscobedoÎncă nu există evaluări
- Complications of Chronic Kidney Disease Current STDocument32 paginiComplications of Chronic Kidney Disease Current STmetaÎncă nu există evaluări
- Acute Kidney Injury-An UpdateDocument99 paginiAcute Kidney Injury-An UpdateProf Brigadier Mamun MostafiÎncă nu există evaluări
- Chronic Kidney Disease Secondary To Type 2 Diabetes MellitusDocument84 paginiChronic Kidney Disease Secondary To Type 2 Diabetes Mellituswar5Încă nu există evaluări
- By B. Shalini Under The Guidance of Neelakant Reddy Patil M.PharmDocument25 paginiBy B. Shalini Under The Guidance of Neelakant Reddy Patil M.PharmShalini Reddy100% (1)
- Predisposing Conditions, Management and Prevention of Chronic Kidney DiseaseDocument52 paginiPredisposing Conditions, Management and Prevention of Chronic Kidney DiseaseSaad MotawéaÎncă nu există evaluări
- Pahtophysiology of EsrdDocument5 paginiPahtophysiology of EsrdCarl JardelezaÎncă nu există evaluări
- CKDDocument35 paginiCKDNATTAPAT SANGKAKULÎncă nu există evaluări
- Hepatomegaly 1Document5 paginiHepatomegaly 1Bobby ParksÎncă nu există evaluări
- GingerDocument10 paginiGingernarenvasagamÎncă nu există evaluări
- Narrative PathophysiologyDocument18 paginiNarrative PathophysiologyNica Georgelle Maniego SamonteÎncă nu există evaluări
- HyperphosphatemiaDocument18 paginiHyperphosphatemiaS.R.Cogo100% (1)
- Hemorrhagic Cerebro Vascular DiseaseDocument37 paginiHemorrhagic Cerebro Vascular Diseasejbvaldez100% (1)
- Drug Induced NephrotoxicityDocument13 paginiDrug Induced NephrotoxicityAgnes BastonÎncă nu există evaluări
- Clinical Pharmacy Lab - Quiz Part 2Document4 paginiClinical Pharmacy Lab - Quiz Part 2Aassh DcmbrÎncă nu există evaluări
- Renal FailureDocument41 paginiRenal Failure12046Încă nu există evaluări
- Overview of The Management of Acute Kidney Injury in Adults - UpToDateDocument13 paginiOverview of The Management of Acute Kidney Injury in Adults - UpToDateDaniely FreitasÎncă nu există evaluări
- Glomerular FiltrationDocument3 paginiGlomerular FiltrationyolandadwiooÎncă nu există evaluări
- Cerebrovascular Accident (CVA)Document71 paginiCerebrovascular Accident (CVA)nur muizzah afifah hussinÎncă nu există evaluări
- AtaxiaDocument23 paginiAtaxiakara_korumÎncă nu există evaluări
- Alawlaqi - Obesity FinalDocument26 paginiAlawlaqi - Obesity FinalMotea Alawlaqi100% (1)
- Glomerulonephritis-1 (Dr. Soffa)Document58 paginiGlomerulonephritis-1 (Dr. Soffa)Rahmailla Khanza Diana FebriliantriÎncă nu există evaluări
- Renal DisordersDocument77 paginiRenal Disorderslorelee_espaldon100% (1)
- Hyporeninemic HypoaldosteronismDocument12 paginiHyporeninemic HypoaldosteronismCésar Augusto Sánchez SolisÎncă nu există evaluări
- CKD Case StudyDocument24 paginiCKD Case Studyapi-384366795Încă nu există evaluări
- Diabetes Mellitus, Often Simply Referred To As Diabetes, Is A Group of Metabolic Diseases inDocument28 paginiDiabetes Mellitus, Often Simply Referred To As Diabetes, Is A Group of Metabolic Diseases inKrissy GaluraÎncă nu există evaluări
- Hyponatremia and Hypernatremia in The ElderlyDocument15 paginiHyponatremia and Hypernatremia in The ElderlyStacey WoodsÎncă nu există evaluări
- Chronic GlomerulonephritisDocument8 paginiChronic GlomerulonephritisDaniel CornerÎncă nu există evaluări
- Phosphate BinderDocument51 paginiPhosphate BinderbedestySÎncă nu există evaluări
- Diabetic NephropathyDocument198 paginiDiabetic Nephropathyapi-3824046100% (2)
- Clinical Practice Guidelines: Management of Type 2 Diabetes Mellitus (5 Edition) 2015Document13 paginiClinical Practice Guidelines: Management of Type 2 Diabetes Mellitus (5 Edition) 2015Azim Abd Razak100% (1)
- Case Presentation - CKDDocument27 paginiCase Presentation - CKDAmanda Padma50% (2)
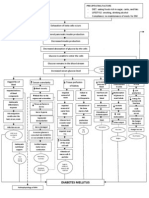
- Pa Tho Physiology of Diabetes MellitusDocument3 paginiPa Tho Physiology of Diabetes MellitusPong's Teodoro SalvadorÎncă nu există evaluări
- Congestive Heart FailureDocument14 paginiCongestive Heart FailureBella Trix PagdangananÎncă nu există evaluări
- A Guide To Hypoparathyroidism PDFDocument16 paginiA Guide To Hypoparathyroidism PDFNurrochmah SitiÎncă nu există evaluări
- Renal Replacement Therapy in Acute Kidney Injury 2017Document14 paginiRenal Replacement Therapy in Acute Kidney Injury 2017piero reyes100% (1)
- MS - Gastroesophageal Reflux DiseaseDocument15 paginiMS - Gastroesophageal Reflux DiseasePrincess Celmea SalongaÎncă nu există evaluări
- HyponatremiaDocument44 paginiHyponatremiaALi TaLib ShukurÎncă nu există evaluări
- Urolithiasis (Renal Calculi)Document12 paginiUrolithiasis (Renal Calculi)jhodane100% (1)
- Hypertension Case StudyDocument2 paginiHypertension Case Studyapi-344630051Încă nu există evaluări
- Presented By: Dr. Hirdesh Chawla Junior Resident IiiDocument79 paginiPresented By: Dr. Hirdesh Chawla Junior Resident IiiAzizan HannyÎncă nu există evaluări
- Department of Kriyasharir: Mahatma Gandhi Ayurved College Hospital & Research Centre Salod (H), WardhaDocument39 paginiDepartment of Kriyasharir: Mahatma Gandhi Ayurved College Hospital & Research Centre Salod (H), WardhaAvanti ShendurjaneÎncă nu există evaluări
- Pathophysiology ErDocument3 paginiPathophysiology ErAlexa A. AldayÎncă nu există evaluări
- Renal Replacement TherapyDocument23 paginiRenal Replacement TherapyShelly Dwi SilvitaÎncă nu există evaluări
- Case 7 ResultsDocument14 paginiCase 7 ResultsRegia putri ellandaÎncă nu există evaluări
- End-Stage Renal Disease: An Integrated ApproachDe la EverandEnd-Stage Renal Disease: An Integrated ApproachWilliam J. StoneÎncă nu există evaluări
- Diabetic Ketoacidosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDe la EverandDiabetic Ketoacidosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsÎncă nu există evaluări
- E Catalogue 2016 PDFDocument28 paginiE Catalogue 2016 PDFAthirah BidinÎncă nu există evaluări
- Alternative Treatment Options in ColorectalDocument7 paginiAlternative Treatment Options in ColorectalAthirah BidinÎncă nu există evaluări
- 24-Ccc Chemo Side EffectsDocument19 pagini24-Ccc Chemo Side EffectsRostina Hardianti AmsyailanÎncă nu există evaluări
- A Review of Revised Sepsis Care BundlesDocument10 paginiA Review of Revised Sepsis Care BundlesAthirah BidinÎncă nu există evaluări
- Ann Occup Hyg 2005 Hedmer 629 37Document9 paginiAnn Occup Hyg 2005 Hedmer 629 37Athirah BidinÎncă nu există evaluări
- Chemotherapy and YouDocument60 paginiChemotherapy and YouYVETTE CLAIRE BORRESÎncă nu există evaluări
- Mass SpectrometryDocument4 paginiMass SpectrometryAthirah BidinÎncă nu există evaluări
- Simvastatin Side Effects in Detail - DrugsDocument8 paginiSimvastatin Side Effects in Detail - DrugsAthirah BidinÎncă nu există evaluări
- Counseling For Gargle, Magic Mouth Wash & Mucositis in Cancer PTDocument3 paginiCounseling For Gargle, Magic Mouth Wash & Mucositis in Cancer PTAthirah BidinÎncă nu există evaluări
- Ethics GuidelinesDocument15 paginiEthics GuidelinesAthirah BidinÎncă nu există evaluări
- Oral Rivaroxaban For The Treatment of Symptomatic Pulmonary EmbolismDocument11 paginiOral Rivaroxaban For The Treatment of Symptomatic Pulmonary EmbolismAthirah BidinÎncă nu există evaluări
- Chemistry Report 1Document6 paginiChemistry Report 1Athirah BidinÎncă nu există evaluări
- Biotechnology 2014Document5 paginiBiotechnology 2014Athirah BidinÎncă nu există evaluări
- Resume FarmakokinetikaDocument6 paginiResume FarmakokinetikaAthirah BidinÎncă nu există evaluări
- Chemistry Report 2Document8 paginiChemistry Report 2Athirah BidinÎncă nu există evaluări
- Size Exclusion ChromatographyDocument3 paginiSize Exclusion ChromatographyAthirah BidinÎncă nu există evaluări
- BioMed PresentationDocument10 paginiBioMed PresentationAthirah BidinÎncă nu există evaluări
- Menstrual CycleDocument6 paginiMenstrual CycleAthirah BidinÎncă nu există evaluări
- ICU Drug ManualDocument442 paginiICU Drug Manualsgod34Încă nu există evaluări
- Tugas BiokimiaDocument1 paginăTugas BiokimiainnamuthiÎncă nu există evaluări
- Chemistry Report 1Document6 paginiChemistry Report 1Athirah BidinÎncă nu există evaluări
- Chemistry Report 1Document6 paginiChemistry Report 1Athirah BidinÎncă nu există evaluări
- Laundry SoftwareDocument2 paginiLaundry SoftwareAthirah BidinÎncă nu există evaluări
- Aspirin InhibitorDocument2 paginiAspirin InhibitorAthirah BidinÎncă nu există evaluări
- Postoperative Pain ManagementDocument43 paginiPostoperative Pain ManagementPingKikiÎncă nu există evaluări
- Adverse Event TemplateDocument5 paginiAdverse Event TemplateGocThuGianÎncă nu există evaluări
- Storage Conditions - Harlan Teklad DietsDocument4 paginiStorage Conditions - Harlan Teklad DietsDinesh LoganathanÎncă nu există evaluări
- s13014 015 0495 4Document6 paginis13014 015 0495 4produxing 101Încă nu există evaluări
- 03 Guidance For Pharmacists On The Safe Supply of Sumatriptan 50mg TabletsDocument4 pagini03 Guidance For Pharmacists On The Safe Supply of Sumatriptan 50mg TabletssefrounfÎncă nu există evaluări
- Static Station: Carefully Look at Given Photograph and Answer The Following QuestionsDocument36 paginiStatic Station: Carefully Look at Given Photograph and Answer The Following QuestionsmomoÎncă nu există evaluări
- 331-Book Chapter-3614-2-10-20210406Document20 pagini331-Book Chapter-3614-2-10-20210406Yolla GitamayaÎncă nu există evaluări
- E ChaptersDocument390 paginiE ChaptersDana IonescuÎncă nu există evaluări
- 43,47 Waste Management StepDocument4 pagini43,47 Waste Management StepSajib BhuiyanÎncă nu există evaluări
- Theoretical Weaknesses Lead To Practical Problems - The Example of Self-Efficacy TheoryDocument9 paginiTheoretical Weaknesses Lead To Practical Problems - The Example of Self-Efficacy TheoryMkt SchrbrÎncă nu există evaluări
- IsoketDocument2 paginiIsoketGuinzaÎncă nu există evaluări
- Three Basic Spring Forest Qigong ExercisesDocument8 paginiThree Basic Spring Forest Qigong Exercisesgaweshajeewani67% (3)
- V2 Reimagine Reconstruction Ligament Brochure Digital 0322Document71 paginiV2 Reimagine Reconstruction Ligament Brochure Digital 0322Juan Martinez Del AngelÎncă nu există evaluări
- Ozone Application in Apple ProcessingDocument2 paginiOzone Application in Apple ProcessingCosimo RocheÎncă nu există evaluări
- Raphex 2010 PDFDocument26 paginiRaphex 2010 PDFcarlosqueiroz7669100% (3)
- Tissue Regeneration and Muscle ToneDocument9 paginiTissue Regeneration and Muscle ToneDokacodeÎncă nu există evaluări
- Slipped Capital Femoral EpiphysisDocument17 paginiSlipped Capital Femoral EpiphysisElvisÎncă nu există evaluări
- Curry Leaves - A Medicinal Herb: ISSN-2231-5683 (Print) ISSN - 2231-5691 (Online)Document3 paginiCurry Leaves - A Medicinal Herb: ISSN-2231-5683 (Print) ISSN - 2231-5691 (Online)Anand Srinivas RamanÎncă nu există evaluări
- James Brooks BME 281 Presentation 1Document12 paginiJames Brooks BME 281 Presentation 1Sumanta BhattacharyyaÎncă nu există evaluări
- Assignment On IMNCIDocument3 paginiAssignment On IMNCIcharanjit kaurÎncă nu există evaluări
- Candida Auris 1690952022Document10 paginiCandida Auris 16909520225n5przwzfsÎncă nu există evaluări
- CC1 Lab. Notes (Carbo)Document5 paginiCC1 Lab. Notes (Carbo)Kimberly Joy GregorioÎncă nu există evaluări
- 10b. Pathogenesis & Pathophysiology of Bleeding Disorders (KELAS B)Document45 pagini10b. Pathogenesis & Pathophysiology of Bleeding Disorders (KELAS B)MUHAMMAD BAGIR ALJUFRIÎncă nu există evaluări
- Cannabis Industry: 2020 Predictions: Cannabis Legalization Is Going GlobalDocument4 paginiCannabis Industry: 2020 Predictions: Cannabis Legalization Is Going GlobalHAS UYARÎncă nu există evaluări
- Wilson (1994) Behavioral Treatment of Obesity. Thirty Years and CountingDocument45 paginiWilson (1994) Behavioral Treatment of Obesity. Thirty Years and CountingGustavo AyalaÎncă nu există evaluări
- PEBC Qualifying Exam References and Resources ListDocument5 paginiPEBC Qualifying Exam References and Resources ListAnkit ShahÎncă nu există evaluări
- Identifying and Correcting Blocked Learning Gates1Document4 paginiIdentifying and Correcting Blocked Learning Gates1ramaaÎncă nu există evaluări
- Fluids and Electrlytes 1Document14 paginiFluids and Electrlytes 1Pau-pau BasiÎncă nu există evaluări
- Effects of Low Level Laser Therapy Vs Ultrasound Therapy in The Management of Active Trapezius Trigger PointsDocument12 paginiEffects of Low Level Laser Therapy Vs Ultrasound Therapy in The Management of Active Trapezius Trigger PointsABIN ABRAHAM MAMMEN (PHYSIOTHERAPIST)Încă nu există evaluări
- Danafarber CancerDocument273 paginiDanafarber CanceriulianamileaÎncă nu există evaluări