S-ar putea să vă placă și
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
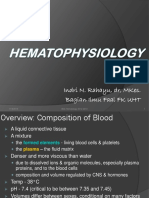
- Hematophysiology 2012-2013Document62 paginiHematophysiology 2012-2013belindaÎncă nu există evaluări
- Chapter 1 - AnswersDocument4 paginiChapter 1 - AnswersthrowawyÎncă nu există evaluări
- ABO Blood Typing: Forward Typing (Glass Slide Method)Document2 paginiABO Blood Typing: Forward Typing (Glass Slide Method)Marj MendezÎncă nu există evaluări
- Richard Hudson's Letter Dated September 12, 2017Document7 paginiRichard Hudson's Letter Dated September 12, 2017WSETÎncă nu există evaluări
- ABO Blood Group System NotesDocument45 paginiABO Blood Group System NotesAnne Carmel Verano100% (1)
- Bio120 Labex12 Genetics 1Document30 paginiBio120 Labex12 Genetics 1api-525858524Încă nu există evaluări
- Non-Mendelian GeneticsDocument11 paginiNon-Mendelian GeneticsalexandriaÎncă nu există evaluări
- Abo and MN Blood Group SystemDocument54 paginiAbo and MN Blood Group SystemAkram chaudaryÎncă nu există evaluări
- CM2-CU10-Modification of Mendelian RatiosDocument17 paginiCM2-CU10-Modification of Mendelian RatiosClaire GonoÎncă nu există evaluări
- Co-Dominance Blood Groups and Rhesus Factor: DR - Mohammed Iqbal Musani, MDDocument38 paginiCo-Dominance Blood Groups and Rhesus Factor: DR - Mohammed Iqbal Musani, MDisasai52Încă nu există evaluări
- Blood TypingDocument3 paginiBlood TypingNoriz Ember DominguezÎncă nu există evaluări
- Package Insert - Biotestcell A1 & B and Biotestcell A2 - 0Document2 paginiPackage Insert - Biotestcell A1 & B and Biotestcell A2 - 0Ahmed AliÎncă nu există evaluări
- 4.05 Virtual Blood Typing / Transfusion Lab Simulation LabDocument3 pagini4.05 Virtual Blood Typing / Transfusion Lab Simulation LabMichael TownsendÎncă nu există evaluări
- Jurnal Nilai Darah, Koagulasi Darah, Golongan Darah, Dan Apusan DarahDocument14 paginiJurnal Nilai Darah, Koagulasi Darah, Golongan Darah, Dan Apusan DarahMela OktavianiÎncă nu există evaluări
- Transfusion Administration Blood ProductsDocument19 paginiTransfusion Administration Blood ProductsEmhemed Amer TabibÎncă nu există evaluări
- Science Quarter 1 Module 4 PDFDocument40 paginiScience Quarter 1 Module 4 PDFshang121182% (11)
- ABO DiscrepanciesDocument40 paginiABO DiscrepanciesAlondra SagarioÎncă nu există evaluări
- SCIENCE-9 Q1 W3 Mod3 ADMDocument35 paginiSCIENCE-9 Q1 W3 Mod3 ADMMönica MasangkâyÎncă nu există evaluări
- Blood Bank ProceduresDocument102 paginiBlood Bank Proceduresahalimyousef70% (10)
- Blood Bank2Document85 paginiBlood Bank22131443Încă nu există evaluări
- InheritanceDocument230 paginiInheritancebiologi88Încă nu există evaluări
- Blood BankDocument19 paginiBlood Bankmoonfire2009100% (2)
- LECTURE 6 The ABO Blood Group SystemDocument64 paginiLECTURE 6 The ABO Blood Group SystemKrisyah Niqoule Valdez100% (2)
- Pointers Prof. Ed. 1 MidtermDocument28 paginiPointers Prof. Ed. 1 MidtermefefÎncă nu există evaluări
- 51 Accidental Inventions That Changed The WorldDocument206 pagini51 Accidental Inventions That Changed The WorldCoates HunterÎncă nu există evaluări
- Blood Grouping (BCS) LDocument10 paginiBlood Grouping (BCS) Ljaish8904Încă nu există evaluări
- Blood and Bodily FluidsDocument6 paginiBlood and Bodily FluidsMaureenÎncă nu există evaluări
- Blood TypesDocument12 paginiBlood Typesapi-277471896Încă nu există evaluări
- Immunology RDNA Bioinformatics ManualDocument60 paginiImmunology RDNA Bioinformatics ManualPrakash BaluÎncă nu există evaluări
- ABO Incompatibility Disease of The NewbornDocument10 paginiABO Incompatibility Disease of The NewbornSha CapiliÎncă nu există evaluări