S-ar putea să vă placă și
- Surface Characteristics ImplantsDocument83 paginiSurface Characteristics ImplantsdrpriyamÎncă nu există evaluări
- Dental Implant FailureDocument71 paginiDental Implant FailureDrIbrahimShaikhÎncă nu există evaluări
- Lecture 17 Dental Implants (Slides)Document34 paginiLecture 17 Dental Implants (Slides)JustDen09100% (1)
- Osseointegration of Bone ImplantsDocument15 paginiOsseointegration of Bone ImplantsBaris BogazkesenliÎncă nu există evaluări
- FACEBOWDocument30 paginiFACEBOWHarini PadmanabhanÎncă nu există evaluări
- Digital Impression 2022Document23 paginiDigital Impression 2022AseelÎncă nu există evaluări
- Scientific Rationale For Dental Implant DesignDocument53 paginiScientific Rationale For Dental Implant DesignM Priya100% (1)
- Basal Osseointegrated Implants ClassificDocument7 paginiBasal Osseointegrated Implants ClassificAnkur SaladaÎncă nu există evaluări
- Articulators, Classification&AdjustmentDocument81 paginiArticulators, Classification&AdjustmentfitsumÎncă nu există evaluări
- 3 D PrintingDocument4 pagini3 D PrintingProsthodontics DeptÎncă nu există evaluări
- Osseointegration and Bone BiologyDocument29 paginiOsseointegration and Bone BiologyHarini PadmanabhanÎncă nu există evaluări
- Jaw Relation Records For Fixed ProsthodonticsDocument16 paginiJaw Relation Records For Fixed ProsthodonticsbkprosthoÎncă nu există evaluări
- Mandibular Anatomical LandmarksDocument14 paginiMandibular Anatomical LandmarksKishor Chindam100% (4)
- Dental Implants - Classification, Success and Failure - An OverviewDocument8 paginiDental Implants - Classification, Success and Failure - An OverviewIOSRjournalÎncă nu există evaluări
- Osteoconduction and OsteoinductionDocument6 paginiOsteoconduction and OsteoinductiontofssbiÎncă nu există evaluări
- A Clinical Overview of Removable Prostheses 3. Principles of Design For Removable Partial DenturesDocument7 paginiA Clinical Overview of Removable Prostheses 3. Principles of Design For Removable Partial DenturesMohsin HabibÎncă nu există evaluări
- Denture Base MaterialDocument100 paginiDenture Base Materialpbhu1Încă nu există evaluări
- Retentive Aids in Maxillofacial ProsthesisDocument109 paginiRetentive Aids in Maxillofacial ProsthesisEnu KambojÎncă nu există evaluări
- Titanium in Dentistry Historical Development State of The Art PDFDocument7 paginiTitanium in Dentistry Historical Development State of The Art PDFPabloÎncă nu există evaluări
- Cad Cam ReviewDocument5 paginiCad Cam ReviewnabeghÎncă nu există evaluări
- 11 Retention of Maxillofacial Prosthesis Fayad PDFDocument7 pagini11 Retention of Maxillofacial Prosthesis Fayad PDFMostafa Fayad50% (2)
- 'The Mettle'' - Recent Advancement in Maxillofacial ProstheticsDocument4 pagini'The Mettle'' - Recent Advancement in Maxillofacial ProstheticsAmaliÎncă nu există evaluări
- Lasers in Prosthodontics The21st CenturyDocument32 paginiLasers in Prosthodontics The21st Centuryaziz2007Încă nu există evaluări
- Horizontal Jaw RelationsDocument90 paginiHorizontal Jaw RelationsKeerthiga TamilarasanÎncă nu există evaluări
- 2022 Bone Graft SubstitutesDocument30 pagini2022 Bone Graft Substitutesemi ala100% (1)
- Removable Partial Dentures PDFDocument6 paginiRemovable Partial Dentures PDFPadmini ReddyÎncă nu există evaluări
- Classification and Impression Techniques of ImplantsDocument72 paginiClassification and Impression Techniques of ImplantsvanillalavenderÎncă nu există evaluări
- Anterior Single Implant Supported Restoration in Esthetic ZoneDocument71 paginiAnterior Single Implant Supported Restoration in Esthetic ZoneAmar BimavarapuÎncă nu există evaluări
- Spacer DesignDocument44 paginiSpacer Designyabhatia100% (1)
- 2006 Implant SurfacesDocument16 pagini2006 Implant SurfacesLukas Lopez RamirezÎncă nu există evaluări
- Acrylic Partial DenturesDocument5 paginiAcrylic Partial DenturesCloudcynaraaÎncă nu există evaluări
- Maxillofacial Defects PDFDocument244 paginiMaxillofacial Defects PDFKirti Sharma100% (5)
- Retention of Maxillofacial Prosthesis PDFDocument6 paginiRetention of Maxillofacial Prosthesis PDFBismita PradhanÎncă nu există evaluări
- Implant SeminarDocument62 paginiImplant SeminarDr. Abdulsalam Awas Dental CenterÎncă nu există evaluări
- Sri Guru Ram Das Institute of Dental Sciences and Research: Impression Techniques For Implant Supported ProsthesisDocument36 paginiSri Guru Ram Das Institute of Dental Sciences and Research: Impression Techniques For Implant Supported Prosthesisgurpreetdentist100% (1)
- Parts of A Dental ImplantDocument28 paginiParts of A Dental Implantdr parveen bathlaÎncă nu există evaluări
- BIOMECHANICS OF DENTAL IMPLANTS FinalDocument57 paginiBIOMECHANICS OF DENTAL IMPLANTS FinalNikita Aggarwal100% (1)
- Bicon Short Implant 1Document6 paginiBicon Short Implant 1Bicon Implant InaÎncă nu există evaluări
- PeekDocument8 paginiPeeksalmaÎncă nu există evaluări
- Selecting and Customzing Implant Abutments For Cemented RestorationsDocument75 paginiSelecting and Customzing Implant Abutments For Cemented RestorationsAnonymous yHCKO5AP100% (1)
- Unit - 1. Overview of BiomaterialsDocument33 paginiUnit - 1. Overview of Biomaterialsronaldo magarÎncă nu există evaluări
- Osseteointegration of Dental ImplantDocument24 paginiOsseteointegration of Dental ImplantFajar Kusuma Dwi KurniawanÎncă nu există evaluări
- Journal Club 5Document74 paginiJournal Club 5Naveen Kumar100% (1)
- Removable Prosthodontics II - Lec.10, Indirect Retainers - Noor Al-Deen M. Al-KhanatiDocument3 paginiRemovable Prosthodontics II - Lec.10, Indirect Retainers - Noor Al-Deen M. Al-KhanatiNoor Al-Deen Maher100% (1)
- Immediate Vs Delayed Implant PlacementDocument60 paginiImmediate Vs Delayed Implant PlacementYashica KalyaniÎncă nu există evaluări
- Prosthodontic Stents: March 2019Document28 paginiProsthodontic Stents: March 2019Ahmad WahabÎncă nu există evaluări
- History of ProsthodonticsDocument121 paginiHistory of ProsthodonticsArthi Ramalingam aÎncă nu există evaluări
- 300 ArticulatorsDocument65 pagini300 Articulatorsthebhaskar100% (1)
- Basic Dental Implant SurgeryDocument33 paginiBasic Dental Implant Surgerymuhammad100% (1)
- OcclusionDocument49 paginiOcclusionRajsandeep SinghÎncă nu există evaluări
- Biological Considerations in Mandibular ImpressionDocument105 paginiBiological Considerations in Mandibular Impressionshraddha100% (1)
- Retentive Aids in Maxillofacial Prosthes PDFDocument4 paginiRetentive Aids in Maxillofacial Prosthes PDFmaha mohÎncă nu există evaluări
- ArticulatorsDocument107 paginiArticulatorsSingh JyotiÎncă nu există evaluări
- Maxillofacial ProsthesisxdfgDocument22 paginiMaxillofacial ProsthesisxdfgbkprosthoÎncă nu există evaluări
- Progressive LoadingDocument86 paginiProgressive LoadingHimani Soni Madaan100% (1)
- Dental Implant OsseointegrationDocument12 paginiDental Implant Osseointegrationdrgayen6042Încă nu există evaluări
- Maxillofacial MaterialsDocument78 paginiMaxillofacial Materialsshweta100% (1)
- Classification of Failure of FPDDocument4 paginiClassification of Failure of FPDrayavarapu sunilÎncă nu există evaluări
- Minimally Invasive Dental Implant SurgeryDe la EverandMinimally Invasive Dental Implant SurgeryDaniel R. CullumÎncă nu există evaluări
- Color & Shade Matching PPT - UnlockedDocument70 paginiColor & Shade Matching PPT - UnlockedAmit Bhargav100% (1)
- Retainer in Fixed Partial Denture'S: 1 Presented by - Dr. Amit Bhargav Post Graduate 3 Year Deptt. of ProsthodonticsDocument29 paginiRetainer in Fixed Partial Denture'S: 1 Presented by - Dr. Amit Bhargav Post Graduate 3 Year Deptt. of ProsthodonticsAmit BhargavÎncă nu există evaluări
- Retainers in FPDDocument153 paginiRetainers in FPDAmit Bhargav88% (8)
- OverdentureDocument97 paginiOverdentureAmit Bhargav100% (1)
- Posterior Palatal Seal ProsthoDocument64 paginiPosterior Palatal Seal ProsthoAmit BhargavÎncă nu există evaluări
- Tilted Post Teeh II Biomech TherapyDocument7 paginiTilted Post Teeh II Biomech TherapyAmit BhargavÎncă nu există evaluări
- Posterior Palatal SealDocument74 paginiPosterior Palatal SealAmit Bhargav50% (2)
- Hollow DenturesDocument31 paginiHollow DenturesAmit BhargavÎncă nu există evaluări
- Anatomy of Head and Neck Nerve Supply and Lymphatic DrainageDocument168 paginiAnatomy of Head and Neck Nerve Supply and Lymphatic DrainageAmit Bhargav100% (3)
- The Effect of Surface Treatment On Fiber ReinforcedDocument28 paginiThe Effect of Surface Treatment On Fiber ReinforcedAmit BhargavÎncă nu există evaluări
- Complete Denture Prosthodontics in Children With Ectodermal DysplasiaDocument29 paginiComplete Denture Prosthodontics in Children With Ectodermal DysplasiaAmit BhargavÎncă nu există evaluări
- Comparative Anatomy of Bone, Brain, Skull, Muskuloskeletal System, Gait and PostureDocument62 paginiComparative Anatomy of Bone, Brain, Skull, Muskuloskeletal System, Gait and PostureAmit BhargavÎncă nu există evaluări
- Cranial Nerves (7 12)Document87 paginiCranial Nerves (7 12)Amit BhargavÎncă nu există evaluări
- Antioxidant Capacity of Some Turkish Pomegranate Genotypes Grown in Siirt RegionDocument6 paginiAntioxidant Capacity of Some Turkish Pomegranate Genotypes Grown in Siirt RegioniajerÎncă nu există evaluări
- Solid-State Welding ProcessesDocument17 paginiSolid-State Welding ProcessescfcshakerÎncă nu există evaluări
- 5354 Greases 2010 03Document6 pagini5354 Greases 2010 03Gajendra SorenÎncă nu există evaluări
- مثال فصل 3Document10 paginiمثال فصل 3mohammadÎncă nu există evaluări
- Vsa 032 - Vsa 068 - Vsa 100 - AuDocument9 paginiVsa 032 - Vsa 068 - Vsa 100 - AuMariana CardosoÎncă nu există evaluări
- CAPE® Chemistry Free ResourcesDocument4 paginiCAPE® Chemistry Free Resourcesabbey4623Încă nu există evaluări
- Water Vapor Capacity of AirDocument3 paginiWater Vapor Capacity of AirAhmed EldalyÎncă nu există evaluări
- MSDS Accelerator MBT 2-Mercaptobenzothiazole KemaiDocument7 paginiMSDS Accelerator MBT 2-Mercaptobenzothiazole KemaicarlosÎncă nu există evaluări
- Friction Welding Usage TodayDocument15 paginiFriction Welding Usage Todaycule93Încă nu există evaluări
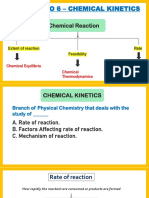
- Chapter No 6 - Chemical KineticsDocument45 paginiChapter No 6 - Chemical KineticsTanish SalviÎncă nu există evaluări
- Emission CharacteristicsDocument48 paginiEmission CharacteristicsBALAJIÎncă nu există evaluări
- Precipitation Hardening: Dr. H. K. Khaira Professor in MSME MANIT, BhopalDocument42 paginiPrecipitation Hardening: Dr. H. K. Khaira Professor in MSME MANIT, Bhopalsatya narayana murthyÎncă nu există evaluări
- Ugiweb 52492Document5 paginiUgiweb 52492badrÎncă nu există evaluări
- Bio Gas Seminar ReportDocument49 paginiBio Gas Seminar ReportLalitBisht100% (2)
- Standard Thermo Data 298 KDocument12 paginiStandard Thermo Data 298 KRebecca FrancisÎncă nu există evaluări
- MCQs All With KeysDocument47 paginiMCQs All With KeysSana UllahÎncă nu există evaluări
- Claytone Af TDS (En)Document2 paginiClaytone Af TDS (En)محمد عزت100% (1)
- QC of SuppositoriesDocument36 paginiQC of Suppositoriesroma imtiazÎncă nu există evaluări
- Bioanalytical Method Validation - ICHDocument3 paginiBioanalytical Method Validation - ICHfdfsdfdssfsfsÎncă nu există evaluări
- Plastics Engineering: Process Equipment and Piping Systems For Optimum Reliability and Cost-EffectivenessDocument9 paginiPlastics Engineering: Process Equipment and Piping Systems For Optimum Reliability and Cost-EffectivenesskoushkiÎncă nu există evaluări
- The Ideal Gas Law and Gas Stoichiometry Hon)Document3 paginiThe Ideal Gas Law and Gas Stoichiometry Hon)Camilo RosasÎncă nu există evaluări
- B1 Distrubutory DesignDocument17 paginiB1 Distrubutory DesignNeil AgshikarÎncă nu există evaluări
- Flown Ex Simulation EnvironmentDocument12 paginiFlown Ex Simulation EnvironmentSanthosh LingappaÎncă nu există evaluări
- Isolation of Acetylsalicylic AcidDocument4 paginiIsolation of Acetylsalicylic AcidPrince Pulvera100% (1)
- 12 - National Cera Lab Test Report - 600x1200 MM - 24.12.2019Document3 pagini12 - National Cera Lab Test Report - 600x1200 MM - 24.12.2019Shaikh MohammedHanifSultanÎncă nu există evaluări
- Solid Fuel SeriesDocument15 paginiSolid Fuel SeriesCesar ValenciaÎncă nu există evaluări
- CEeNews2 04Document6 paginiCEeNews2 04Antonio MezzopreteÎncă nu există evaluări
- Din 1690Document7 paginiDin 1690saravananÎncă nu există evaluări
- Chemistry Viva QuestionsDocument3 paginiChemistry Viva QuestionsShivamÎncă nu există evaluări
- Bacte Comprehensive ReviewDocument116 paginiBacte Comprehensive ReviewFaith Theresa OroscoÎncă nu există evaluări