S-ar putea să vă placă și
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- New Guidelines On Nonstatin Lipid Lowering 2016-8-16Document7 paginiNew Guidelines On Nonstatin Lipid Lowering 2016-8-16micheal1960Încă nu există evaluări
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- A Better Test Than HbA1c Oct 19, 2016Document5 paginiA Better Test Than HbA1c Oct 19, 2016micheal1960Încă nu există evaluări
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Kid StonesDocument5 paginiKid Stonesmicheal1960Încă nu există evaluări
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Lipid Lowering With Statin Is Better Than Adding Other AgentDocument1 paginăLipid Lowering With Statin Is Better Than Adding Other Agentmicheal1960Încă nu există evaluări
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (894)
- Taylors.10 Minute - Diagnosis.manual - Symptoms.and - Signs.in - The.time Limited - Encounter.Document656 paginiTaylors.10 Minute - Diagnosis.manual - Symptoms.and - Signs.in - The.time Limited - Encounter.micheal1960Încă nu există evaluări
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- AKI MGMT 2005-11-1 AAFP p1739Document8 paginiAKI MGMT 2005-11-1 AAFP p1739micheal1960Încă nu există evaluări
- Normal ValuesDocument6 paginiNormal ValuesMc Crister SilangÎncă nu există evaluări
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Normal ValuesDocument6 paginiNormal ValuesMc Crister SilangÎncă nu există evaluări
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- 13 Can'T-Miss Findings On Pediatric Imaging 2015-12-2Document29 pagini13 Can'T-Miss Findings On Pediatric Imaging 2015-12-2micheal1960Încă nu există evaluări
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (587)
- MBF2306162Document137 paginiMBF2306162DrHassan Ahmed ShaikhÎncă nu există evaluări
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (265)
- Simple Depression Anxiety 2 Simple Screenin QuestionsDocument2 paginiSimple Depression Anxiety 2 Simple Screenin Questionsmicheal1960Încă nu există evaluări
- Serotonin SyndromeDocument5 paginiSerotonin Syndromemicheal1960Încă nu există evaluări
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- Tests Distinguish Pneumonia Types in MinutesDocument3 paginiTests Distinguish Pneumonia Types in Minutesmicheal1960100% (1)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- ABX Common Effects of Antibiotics On Other Drugs MMDocument3 paginiABX Common Effects of Antibiotics On Other Drugs MMmicheal1960Încă nu există evaluări
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Low SodiumDocument4 paginiLow Sodiummicheal1960Încă nu există evaluări
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Ezetimibe Simvastatin Post-Acute Coronary SyndromeDocument12 paginiEzetimibe Simvastatin Post-Acute Coronary Syndromemicheal1960Încă nu există evaluări
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Anal Cancer 2016-2-9Document17 paginiAnal Cancer 2016-2-9micheal1960Încă nu există evaluări
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2219)
- RaynaudDocument11 paginiRaynaudmicheal1960Încă nu există evaluări
- Iron Deficiency Anemia 2007-3-1 AAFP p671Document8 paginiIron Deficiency Anemia 2007-3-1 AAFP p671micheal1960Încă nu există evaluări
- Cold Agglutinin Disease 2015-4-28Document9 paginiCold Agglutinin Disease 2015-4-28micheal1960Încă nu există evaluări
- Nail Diseases, Hand in Diagnosis, Terry's NailDocument35 paginiNail Diseases, Hand in Diagnosis, Terry's Nailmicheal1960Încă nu există evaluări
- Trigeminal N Tables SummaryDocument14 paginiTrigeminal N Tables Summarymicheal1960Încă nu există evaluări
- Clinical Challenge Bright Plaques, Papules On The ThumbDocument4 paginiClinical Challenge Bright Plaques, Papules On The Thumbmicheal1960Încă nu există evaluări
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Rheumatoid Arthritis 2015-6-9Document22 paginiRheumatoid Arthritis 2015-6-9micheal1960Încă nu există evaluări
- RaynaudDocument11 paginiRaynaudmicheal1960Încă nu există evaluări
- AF & Oral Anticoagulants 2016Document11 paginiAF & Oral Anticoagulants 2016micheal1960100% (1)
- Athlete's Heart or Cardiomyopathy 2016-3-1Document2 paginiAthlete's Heart or Cardiomyopathy 2016-3-1micheal1960Încă nu există evaluări
- Superficial Venous Insufficiency 2015-6-4Document16 paginiSuperficial Venous Insufficiency 2015-6-4micheal1960Încă nu există evaluări
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (119)
- Prostate Cancer 2015-5-7Document27 paginiProstate Cancer 2015-5-7micheal1960Încă nu există evaluări
- Malabsorption SyndromeDocument7 paginiMalabsorption SyndromePrince AhmedÎncă nu există evaluări
- BetterYou Intra-Oral Spray Research Document2Document3 paginiBetterYou Intra-Oral Spray Research Document2JohnÎncă nu există evaluări
- MCQ Block 13Document15 paginiMCQ Block 13Liliana Surya Fatimah0% (1)
- Disorders of Intestinal AbsorptionDocument83 paginiDisorders of Intestinal AbsorptionMalika SadridinovaÎncă nu există evaluări
- Case Study 17Document5 paginiCase Study 17api-27655178367% (3)
- Anatomy & Physiology of the Digestive SystemDocument29 paginiAnatomy & Physiology of the Digestive Systembeni kurniawanÎncă nu există evaluări
- Graha Roga'sDocument10 paginiGraha Roga'srohinibrajole123Încă nu există evaluări
- Medsurg 1Document59 paginiMedsurg 1Angel YN Patricio FlorentinoÎncă nu există evaluări
- Anemia Types Causes SymptomsDocument9 paginiAnemia Types Causes SymptomsShine Reyes MackieÎncă nu există evaluări
- Malabsorption SyndromeDocument1 paginăMalabsorption SyndromesamanthaÎncă nu există evaluări
- "Nagtatae Siya 4 Days Na" As Verbalized by The Mother. Inatake of Causative Agents Irritation of The Stomach Inflammation of The Stomach Increase GI Motility DiarrrheaDocument4 pagini"Nagtatae Siya 4 Days Na" As Verbalized by The Mother. Inatake of Causative Agents Irritation of The Stomach Inflammation of The Stomach Increase GI Motility DiarrrheaMelissa MhelÎncă nu există evaluări
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Nutrition Support of Children With Chronic LiverDocument14 paginiNutrition Support of Children With Chronic LiverMarcia SchneiderÎncă nu există evaluări
- OTC Exam 2 Study GuideDocument32 paginiOTC Exam 2 Study GuideDave WinÎncă nu există evaluări
- I. Common GI Presentations.: 1. The MouthDocument26 paginiI. Common GI Presentations.: 1. The MouthFarah FarahÎncă nu există evaluări
- An Approach To Failure To Thrive': GrowthDocument5 paginiAn Approach To Failure To Thrive': GrowthJayantiÎncă nu există evaluări
- Case Study Celiac DiseaseDocument8 paginiCase Study Celiac Diseaseapi-242376719Încă nu există evaluări
- Disturbances of Gastrointestinal Tract (Git) : Alzbeta - Trancikova@Jfmed - Uniba.SkDocument57 paginiDisturbances of Gastrointestinal Tract (Git) : Alzbeta - Trancikova@Jfmed - Uniba.SkCharm MeelÎncă nu există evaluări
- Boala Crohn Clinical ManifestationsDocument16 paginiBoala Crohn Clinical ManifestationsEdith CroitoruÎncă nu există evaluări
- Adult Enteral Formula: Presented By: SAMAHER ALSADHANDocument31 paginiAdult Enteral Formula: Presented By: SAMAHER ALSADHANdeliana rahmi rahayuÎncă nu există evaluări
- KNH 411 Case Study 11Document20 paginiKNH 411 Case Study 11api-301897220Încă nu există evaluări
- 7anemia Caused by Defects of DNA MetabolismDocument30 pagini7anemia Caused by Defects of DNA MetabolismanonacadsÎncă nu există evaluări
- Diagnosis-Pedrosa, Joan ADocument27 paginiDiagnosis-Pedrosa, Joan AJoan Alde PedrosaÎncă nu există evaluări
- Juhairina: Medical Nutrition Therapy For Disorders of The Lower Gastrointestinal TractDocument82 paginiJuhairina: Medical Nutrition Therapy For Disorders of The Lower Gastrointestinal Tractdesy100% (1)
- 33818329: Fructose Malabsorption Causes, Diagnosis and TreatmentDocument19 pagini33818329: Fructose Malabsorption Causes, Diagnosis and TreatmentMércia FiuzaÎncă nu există evaluări
- New Celiac DiseaseDocument29 paginiNew Celiac Diseaseapi-203339953Încă nu există evaluări
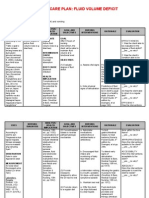
- NCP-Fluid Volume DeficitDocument2 paginiNCP-Fluid Volume Deficitjava_biscocho122979% (33)
- Robert F Kushner - Christopher D Still - Nutrition and Bariatric Surgery (2014, Taylor & Francis, CRC Press) PDFDocument298 paginiRobert F Kushner - Christopher D Still - Nutrition and Bariatric Surgery (2014, Taylor & Francis, CRC Press) PDFLucas PabloÎncă nu există evaluări
- Case Study 11Document28 paginiCase Study 11api-301883277Încă nu există evaluări
- Bariatric Case StudyDocument11 paginiBariatric Case Studyapi-346620455100% (3)
- MFN-005 Unit-14Document46 paginiMFN-005 Unit-14vijayalakshmi gkÎncă nu există evaluări