DIARRHEA
Presented
By
Dwi aprila putri
12-083
DEFINITION
Diarrhea may be defined on the basis of
quantity, frequency and consistency of the
Stools
>200-300 gm/day
>3 stools/day
Unformed liquid stools
CLASSIFICATION
Acute Diarrhea
- Non-inflammatory
- Inflammatory
Chronic Diarrhea
- Osmotic
- Secretary
- Malabsorption
- Inflammatory Infectious Motility disorders
factitious
ACUTE DIARRHEA
Sudden onset
Persists < 2weeks
Most commonly due to
- infections
- toxins
- drugs
AC NON-INFLAMMATORY DIARRHEA
Watery
No blood
No fever Involves small intestine
Voluminous/nausea/vomiting
Peri-umblical pain
Cause hypokalemia & acidosis
No fecal leukocytes
AC NON-INFLAMMATORY DIARRHEA
Caused by
Toxin producing bacteria
- Staph aureus
- Bacillus cereus
- Cl perfrengens
- ETEC (Enterotoxigenic E coli)
Viruses Rotavirus, Norovirus
Protozoal Giardia,Cryposporidium,Cyclospora
AC INFLAMMATORY DIARRHEA
Bloody
Fever
Large bowel involvement
Small in quantity - < 1litre
Left lower quadrant cramps
Urgency
Tenesmus
Faecal leukocytes/lactoferrin
AC INFLAMMATORY DIARRHEA
Viral CMV
Protozoal Entamoeba histolytica
Cytotoxin producing bacteria
- EHEC (Enterohemorrhagic E coli)
- Vibrio parahaemolyticus
- Clostridium difficile
Mucosal invading bacteria
- Shigella
- Salmonella
- Campylobacter jejuni
- EIEC (Enteroinvasive E coli)
- Aeromonas
- Plesiomonas
- Yersinia
- Chlamydia
DIAGNOSIS OF ACUTE DIARRHEA
HISTORY
- See under chronic diarrhea
PHYSICAL EXAMINATION
- See under chronic diarrhea
INVESTIGATIONS
ACUTE DIARRHOEA - INVESTIGATIONS
Stools
- Microscopy
- Antigen
* Giardia
* E histolytica
- Acid staining
* Cryptosporidium
* Cyclospora
- Culture sensitivity not usually required
TREATMENT
Diet
- Avoid high fiber diet, caffeine, alcohol
Rehydration oral or intravenous
- 50-200ml/kg/day of ORS or Ringers lactate
Antidiarrheal agents
- In non-inflammatory diarrhea
- Loperamide in mild/moderat diarrhea
- Anticholinergic agents are CONTRAINDICATED
Toxic Megacolon
Antibiotics
- In inflammatory diarrhea only
CHRONIC DIARRHEA
Osmotic Diarrhea
- Increased osmotic gap > 125mosm/kg (N= up to
50mosm/kg)
- Due to
* Ingestion of osmotically active substance
* Malabsorption
- Resolves during fasting
- Occurs with
* Disaccharidase deficiency viral infection,GIT
surgery
* Laxatives
* Malabsorption syndrome
CHRONIC DIARRHEA
Secretary
Diarrhea
Increased GI secretions
Decreased absorption
Normal osmotic gap
Fasting does not improve condition
Due to
- Endocrine tumours
- Bile salt malabsorption
- Laxatives
CHRONIC DIARRHEA
Inflammatory Diarrhea
- Fever
- Hematochazia
- Examples are
* Ulcerative colitis
* Crohens disease
* Microscopic colitis
CHRONIC DIARRHEA
Malabsorptive
- Weight loss prominent feature
- Deficiency diseases
* Vitamins
* Minerals
- Due to
* Intestinal mucosal disease
* Lymphatic obstruction
* Bacterial overgrowth
CHRONIC DIARRHEA
Motility Disorders
- Rapid transit of food
- Stasis of intestinal contents
- Example Irritable
* Bowel
* Syndrome
CHRONIC DIARRHEA
Chronic Infections
- Parasitic
*Protozoal giardia, E. histolytica
* Cyclospora
- Bacterial
* Aeromonas
* Plesiomonas
- Immunocompromised
* CMV
* MAC
* Isospora
* Cryptosporidium
CHRONIC DIARRHEA
Factitious Diarrhea
- Dilution of stools with
* Urine
* Water
- Laxatives
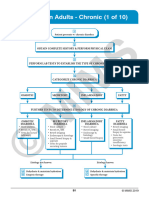
DIAGNOSIS/EVALUATION
History
Physical Examination
Investigations
HISTORY TAKING
What is the complaint
Onset sudden? Gradual?
Duration days ? Weeks? Chronic?
Frequency of stools
Consistency of stools
Any mucus or blood in stools
Fever
Tenesmus
Abdominal cramps peri-umblical? Left lower quadrant?
Food taken
History of gastroenteritis in others sharing same food
Water source
Related to any special food or history of food allergy
History of weight loss
History of abdominal surgery
Any known systemic disease
Features of systemic diseases like
- Relating to thyroid gland
- Relating to carcinoid syndrome
- Relating to malabsorption
- Anxiety / depression
PHYSICAL EXAMINATION
Demeanor
Level of hydration
- Look for tongue
- Sunken eyes
- Skin turger
Temperature, Blood pressure, Pulse rate
Anxious / Depressed / Fidgety
Pallor
Cachexia
Other features of malnourishment
Tremors
Tachycardia
Flushing of face
Abdominal tenderness
Features of liver / pancreatic disease
Other features of relevant systemic diseases
INVESTIGATIONS
24 Hour Stool
- > 300gm indicates diarrhea
- > 500gm excludes IBS
- >1000-1500gm suggests secretary diarrhea
- > 10gm of faecal fat - malabsorption
Stool Osmolality
- < Serum osmolality factitious diarrhea
INVESTIGATIONS
Stool pH < 5.6 - carbohydrate malabsorption
Faecal leukocytes/lactoferin inflammatory
Fecal ova/parasites
- Giardia/E.histolytica
Fecal antigen
- Giardia/E.histolytica
Acid fast staining
- Cryptosporidium/cyclospora
INVESTIGATIONS
Other tests
- CBC
- S.Electrolytes
- LFTs
- Ca++/phosphate
- TSH
- Albumin malabsorption,protein losing
enteropathy
- PTH
- Folate/B12
- Decreased Na+ & nonanion gap met acidosis
secretary diarrhea
INVESTIGATIONS
Specific tests
- Ig G/Ig A antigliadin antibodies celiac sprue
- T tG antibodies celiac sprue
- Serum VIP VIPoma
- Calcitonin medulary thyroid carcinoma
- Gastrin Zollinger-Ellison Syndrome
- Urine for 5HIAA Carcinoid syndrome
- Urine for VMA/Metanephrine -
pheochromocytoma
INVESTIGATIONS
Specific tests
- Endoscopy & Biopsy
* Upper GI tract
* Lower GI tract
- Breath test
* Bacterial overgrowth
- X ray abdomen
* Pancreatic calcification Ch. Pancreatitis
- Barium Radiology
TREATMENT
TREATMENT OF CHRONIC DIARRHEA
IS ACCORDING TO
THE UNDERLYING CAUSE
PRESENTATION ENDS
S-ar putea să vă placă și
- CCRN-PCCN Review GastrointestinalDocument23 paginiCCRN-PCCN Review GastrointestinalGiovanni MictilÎncă nu există evaluări
- Register Environmental ImpactsDocument7 paginiRegister Environmental ImpactsArmand LiviuÎncă nu există evaluări
- Liver Cirrhosis, A Simple Guide To The Condition, Treatment And Related DiseasesDe la EverandLiver Cirrhosis, A Simple Guide To The Condition, Treatment And Related DiseasesÎncă nu există evaluări
- Psychological Aspects of Stress and Adaptation - AmolDocument12 paginiPsychological Aspects of Stress and Adaptation - Amoldanimon1984Încă nu există evaluări
- Honey Nut Baklava Filo Pastry TreatsDocument2 paginiHoney Nut Baklava Filo Pastry TreatsiantperÎncă nu există evaluări
- Human Persons As Oriented Towards Their Impendeing DeathDocument28 paginiHuman Persons As Oriented Towards Their Impendeing DeathMaxwell LaurentÎncă nu există evaluări
- MEO Orals On Marine Electro Technology Function 5Document19 paginiMEO Orals On Marine Electro Technology Function 5Rajeev ValunjkarÎncă nu există evaluări
- Hepatobiliary DiseaseDocument60 paginiHepatobiliary DiseaseFirdaus AslamÎncă nu există evaluări
- Urine Analysis FinalDocument112 paginiUrine Analysis FinalNischita JayarajÎncă nu există evaluări
- DiarrheaDocument41 paginiDiarrheaRia Puji PangestutiÎncă nu există evaluări
- Case Study - BronchopneumoniaDocument45 paginiCase Study - Bronchopneumoniazeverino castillo91% (33)
- GIT DisordersDocument171 paginiGIT DisordersKatrina PonceÎncă nu există evaluări
- Malabsorption: Causes, Symptoms, and TreatmentDocument75 paginiMalabsorption: Causes, Symptoms, and TreatmentLaith Al TamimiÎncă nu există evaluări
- D. G.IDocument23 paginiD. G.IGloryJane100% (1)
- Ricardo A. Caicedo, MD: Pediatric Gastroenterology University of FloridaDocument20 paginiRicardo A. Caicedo, MD: Pediatric Gastroenterology University of FloridaAsma SikanderÎncă nu există evaluări
- TYPHOID FEVER: CAUSES, SYMPTOMS AND TREATMENTDocument48 paginiTYPHOID FEVER: CAUSES, SYMPTOMS AND TREATMENTmanibharathiÎncă nu există evaluări
- Infectious Diarrhea Mechanisms and EtiologyDocument75 paginiInfectious Diarrhea Mechanisms and EtiologyFany Raihan PadilahÎncă nu există evaluări
- Chronic Diarrhea and Malabsorption: Causes and TreatmentDocument25 paginiChronic Diarrhea and Malabsorption: Causes and TreatmentadelekeyusufÎncă nu există evaluări
- Pitri - GI.Pemicu 4. GE+ Tifus AbdominalisDocument154 paginiPitri - GI.Pemicu 4. GE+ Tifus AbdominalisCunCunAlAndraÎncă nu există evaluări
- Chronic DiarrheaDocument38 paginiChronic DiarrheaShujina ZainabÎncă nu există evaluări
- Fecalysis: Verian John Hoo - Sudario College of Medical TechnologyDocument58 paginiFecalysis: Verian John Hoo - Sudario College of Medical Technologyepson printerÎncă nu există evaluări
- DIARRHEA Final Group 8Document65 paginiDIARRHEA Final Group 8angela marie abadillaÎncă nu există evaluări
- 1 Approach To DiarrheaDocument37 pagini1 Approach To DiarrheamusabÎncă nu există evaluări
- Acute Gastroenteritis in ChildhoodDocument39 paginiAcute Gastroenteritis in Childhoodslicvic169Încă nu există evaluări
- Chronic Diarrhea-HTKDocument63 paginiChronic Diarrhea-HTKcerenblgstrÎncă nu există evaluări
- Chronic DiarrheaDocument66 paginiChronic DiarrheaJulita Yanti100% (1)
- Persistent Diarrhoea & Chronic DiarrhoeaDocument34 paginiPersistent Diarrhoea & Chronic DiarrhoeanilmbbsÎncă nu există evaluări
- Gastrointestinal Bleeding Causes, Symptoms and TreatmentDocument84 paginiGastrointestinal Bleeding Causes, Symptoms and TreatmentAngela Kristiana IntanÎncă nu există evaluări
- Seminar Vomit Diarrhea DehydrationDocument71 paginiSeminar Vomit Diarrhea DehydrationrmnordinÎncă nu există evaluări
- Chronic Diarrhea Kuliah Pakar UnissulaDocument27 paginiChronic Diarrhea Kuliah Pakar UnissulaLuthfan HakimÎncă nu există evaluări
- Week 7 - Pediatric GI DisturbancesDocument59 paginiWeek 7 - Pediatric GI DisturbancesLeyla GalyanoÎncă nu există evaluări
- Problem 1: Stefan Satria Group 4Document49 paginiProblem 1: Stefan Satria Group 4Andre OrgantoÎncă nu există evaluări
- Kuliah Melabsorbsi UnizarDocument165 paginiKuliah Melabsorbsi UnizarOpi SaNg MadRidistasÎncă nu există evaluări
- Approach To GI DisordersDocument28 paginiApproach To GI DisordersdrvivekshimlaÎncă nu există evaluări
- GIT 2021 Lect17Document49 paginiGIT 2021 Lect17Nikkole PhalulaÎncă nu există evaluări
- Ulcerative ColitisDocument18 paginiUlcerative ColitisKyle Ü D. CunanersÎncă nu există evaluări
- Gastrointestinal System Symptoms and Signs of Gastrointes Tinal ProblemsDocument77 paginiGastrointestinal System Symptoms and Signs of Gastrointes Tinal ProblemsSindhu BabuÎncă nu există evaluări
- Pemicu 3 GITDocument143 paginiPemicu 3 GITMudita DewiÎncă nu există evaluări
- Diabetes InsipidusDocument11 paginiDiabetes InsipidusAnil Yadav100% (1)
- Diarrhea PPTDocument82 paginiDiarrhea PPTIshwar HavaragiÎncă nu există evaluări
- Lesson 15 Fecalysis and Gastric AnalysisDocument39 paginiLesson 15 Fecalysis and Gastric AnalysisFaith TambongÎncă nu există evaluări
- Diarrhoeal Diseases: A Seminar Presentation by (Renal Unit) Medical Students DATE: December 2013Document43 paginiDiarrhoeal Diseases: A Seminar Presentation by (Renal Unit) Medical Students DATE: December 2013Chinedu H. DuruÎncă nu există evaluări
- Renal Tubules Modify Glomerular Filtrate: Reabsorption of High Threshold SubstancesDocument44 paginiRenal Tubules Modify Glomerular Filtrate: Reabsorption of High Threshold SubstancesajaysomÎncă nu există evaluări
- HAND OUTS ON DIARRHOEA MANAGEMENTDocument14 paginiHAND OUTS ON DIARRHOEA MANAGEMENTNamun Sibora BoraÎncă nu există evaluări
- Kuliah Diare KronikDocument19 paginiKuliah Diare KronikMae Importers IncÎncă nu există evaluări
- Student Copy of Gastrointestinal Problems SP 2010 IggyDocument80 paginiStudent Copy of Gastrointestinal Problems SP 2010 IggyJade CentinoÎncă nu există evaluări
- CHRONIC DIRRHEA FinalDocument93 paginiCHRONIC DIRRHEA FinalAtifÎncă nu există evaluări
- Gastroenterology: Ammad Mahmood GUMSA Revision LecturesDocument49 paginiGastroenterology: Ammad Mahmood GUMSA Revision LecturesgumsaÎncă nu există evaluări
- Acute If 4 Weeks in DurationDocument9 paginiAcute If 4 Weeks in DurationSalsabila Rahma FadlillahÎncă nu există evaluări
- Acute Gastroenteritis in ChildrenDocument39 paginiAcute Gastroenteritis in ChildrenIra Mikkaella GenobisÎncă nu există evaluări
- Chronic Diarrhea Differential Diagnosis and TreatmentDocument37 paginiChronic Diarrhea Differential Diagnosis and TreatmentAzima AyobÎncă nu există evaluări
- Diare Akut Pada Dewasa: Departemen Ilmu Penyakit Dalam FK UsuDocument37 paginiDiare Akut Pada Dewasa: Departemen Ilmu Penyakit Dalam FK Usuardi anharaksa yusuf100% (1)
- GlomerulonefritisDocument43 paginiGlomerulonefritisdian nofitaÎncă nu există evaluări
- Infcetions Intestinal Protozoal InfectionsDocument40 paginiInfcetions Intestinal Protozoal InfectionsDr.P.NatarajanÎncă nu există evaluări
- Small and Large IntestineDocument124 paginiSmall and Large IntestinemariahemnksÎncă nu există evaluări
- Diarrhea: Dr. Ali A. Ramadhan M.B.CH.B., Fibms, Fkbms (G & H)Document27 paginiDiarrhea: Dr. Ali A. Ramadhan M.B.CH.B., Fibms, Fkbms (G & H)Ahmed NazarÎncă nu există evaluări
- Glomerular Filtrate: - Water - Crystalloids - Uric Acid - Proteins With Low Mol. Wt. E.G. HB, Myohb, BJ ProteinsDocument42 paginiGlomerular Filtrate: - Water - Crystalloids - Uric Acid - Proteins With Low Mol. Wt. E.G. HB, Myohb, BJ ProteinsajaysomÎncă nu există evaluări
- Kidney Function and Urine AnalysisDocument42 paginiKidney Function and Urine AnalysisajaysomÎncă nu există evaluări
- Acute and Chronic DiarrhoeaDocument20 paginiAcute and Chronic DiarrhoeaVipul Nagnesia100% (2)
- Gastrointestinal Problems: Dr. Rabie GabrielDocument32 paginiGastrointestinal Problems: Dr. Rabie GabrielRasheed AliÎncă nu există evaluări
- Malabsorption Syndromes in Children PDFDocument6 paginiMalabsorption Syndromes in Children PDFkoreswilsonÎncă nu există evaluări
- Acute GastroEnteritisDocument27 paginiAcute GastroEnteritisRahul MandhanÎncă nu există evaluări
- Acute GastroenteritisDocument48 paginiAcute Gastroenteritisansam kamalÎncă nu există evaluări
- Lecture Diarrhea and ConstipationDocument63 paginiLecture Diarrhea and ConstipationKrittin NaravejsakulÎncă nu există evaluări
- 62 DiarrheaChronic MGHG MIMG MFM 20161229Document10 pagini62 DiarrheaChronic MGHG MIMG MFM 20161229Wei HangÎncă nu există evaluări
- Salmonellasis Typhoid Fever Campylobacter Jejuni Yersinosis ShigellosisDocument5 paginiSalmonellasis Typhoid Fever Campylobacter Jejuni Yersinosis ShigellosisFarhana Azmira AsmadiÎncă nu există evaluări
- Respiratory Epithelium: Human Histology Lecture Chapter 17 Ï The Respiratory SystemDocument16 paginiRespiratory Epithelium: Human Histology Lecture Chapter 17 Ï The Respiratory SystemEvandie OngÎncă nu există evaluări
- Chapter 1 EconomicsDocument5 paginiChapter 1 Economicsjordan cedeñoÎncă nu există evaluări
- Wastewater Collection Systems Comparison: William T. Hensley, International Territory Manager, Orenco Systems, IncDocument5 paginiWastewater Collection Systems Comparison: William T. Hensley, International Territory Manager, Orenco Systems, IncmeskbÎncă nu există evaluări
- Forensic Science Project Group B5518Document5 paginiForensic Science Project Group B5518Anchit JassalÎncă nu există evaluări
- Safety Toolbox Project ProposalDocument33 paginiSafety Toolbox Project ProposalShaffizi Boboy100% (1)
- Liu030 Nepal Bans Solo Mountain ClimbersDocument2 paginiLiu030 Nepal Bans Solo Mountain Climberssanti.miranda.parrillaÎncă nu există evaluări
- Lembar Latihan - P1 - PD MitraDocument123 paginiLembar Latihan - P1 - PD MitratiengcityÎncă nu există evaluări
- Spiegel Et Al 1999 Psycho OncologyDocument12 paginiSpiegel Et Al 1999 Psycho Oncologyfatimaramos31Încă nu există evaluări
- LAOKEN Comparison With J&JDocument3 paginiLAOKEN Comparison With J&JMario Alfonso MartinezÎncă nu există evaluări
- Product and Service Costing: Job-Order System: Questions For Writing and DiscussionDocument22 paginiProduct and Service Costing: Job-Order System: Questions For Writing and Discussionsetiani putriÎncă nu există evaluări
- Ib Items: PotionsDocument8 paginiIb Items: PotionsZeNoWTFÎncă nu există evaluări
- INTUSSUSCEPTIONDocument1 paginăINTUSSUSCEPTIONMaecy PasionÎncă nu există evaluări
- Bar7 Menu 2023Document24 paginiBar7 Menu 2023Diana GamoteÎncă nu există evaluări
- Airtel's Africa Growth: Surviving CompetitionDocument9 paginiAirtel's Africa Growth: Surviving CompetitionSagar RiazÎncă nu există evaluări
- Metals and Metallurgy: Theodore L. Brown H. Eugene Lemay, Jr. and Bruce E. BurstenDocument43 paginiMetals and Metallurgy: Theodore L. Brown H. Eugene Lemay, Jr. and Bruce E. BurstenDheeraj KumarÎncă nu există evaluări
- Samsung Un40c5000 Un46c5000 QF Chassis N98aDocument114 paginiSamsung Un40c5000 Un46c5000 QF Chassis N98ajosue otonielÎncă nu există evaluări
- Shavuot 5774Document4 paginiShavuot 5774Andrea KingÎncă nu există evaluări
- Children's Test Anxiety Scale (CTASDocument10 paginiChildren's Test Anxiety Scale (CTASSchahyda ArleyÎncă nu există evaluări
- Cloudsoc For Amazon Web Services Solution Overview enDocument6 paginiCloudsoc For Amazon Web Services Solution Overview enmanishÎncă nu există evaluări
- Ramdump Modem 2023-05-13 21-52-06 PropsDocument21 paginiRamdump Modem 2023-05-13 21-52-06 PropsNanda TampanÎncă nu există evaluări
- Navi Cure prospectus summaryDocument50 paginiNavi Cure prospectus summaryGaurav SrivastavaÎncă nu există evaluări
- Presentation On: Perfetti Van MelleDocument20 paginiPresentation On: Perfetti Van MelleAkash RaiÎncă nu există evaluări
- NPD High Level Status: Concept Development FeasibilityDocument22 paginiNPD High Level Status: Concept Development FeasibilityRaviÎncă nu există evaluări
- Properties of X-Rays and Gamma RaysDocument13 paginiProperties of X-Rays and Gamma RaysjishnusajiÎncă nu există evaluări