S-ar putea să vă placă și
- A System of Operative Surgery, Volume IV (of 4)De la EverandA System of Operative Surgery, Volume IV (of 4)Evaluare: 4 din 5 stele4/5 (1)
- Abdominal Compartment SyndromeDocument24 paginiAbdominal Compartment SyndromePrateek Vaswani100% (1)
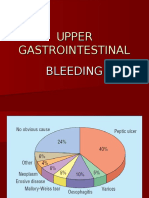
- Upper Gastrointestinal Bleeding.Document13 paginiUpper Gastrointestinal Bleeding.Gieselle Scott100% (1)
- Abdominal Compartment SyndromeDocument22 paginiAbdominal Compartment SyndromeHalbana Al MaududyÎncă nu există evaluări
- Abdominal Compartment SyndromeDocument9 paginiAbdominal Compartment SyndromeNina Kharima100% (1)
- Upper Gastrointestinal Bleeding: Anthony Alexander University of The West Indies at MonaDocument40 paginiUpper Gastrointestinal Bleeding: Anthony Alexander University of The West Indies at MonaAy Alex0% (1)
- CHOLEDOCHOLITHIASISDocument38 paginiCHOLEDOCHOLITHIASISPrecious Cofreros100% (3)
- Abdominal Compartment SyndromeDocument23 paginiAbdominal Compartment SyndromeUmar Farooq GondalÎncă nu există evaluări
- Upper Gi BleedingDocument35 paginiUpper Gi Bleedingnawriirwan100% (1)
- Perforated Gastric UlcerDocument18 paginiPerforated Gastric UlcerNorshahidah IedaÎncă nu există evaluări
- Fat EmbolismDocument12 paginiFat EmbolismHastina HadnanÎncă nu există evaluări
- Hypovolemic ShockDocument2 paginiHypovolemic ShocklarklowÎncă nu există evaluări
- CholelithiasisDocument37 paginiCholelithiasisbaby padzÎncă nu există evaluări
- Upper Gi BleedingDocument35 paginiUpper Gi BleedingAnggreini Susanti100% (2)
- Intestinal ObstructionDocument27 paginiIntestinal ObstructionAna AvilaÎncă nu există evaluări
- Urolithiasis PowerpointDocument41 paginiUrolithiasis PowerpointPinkrose Chiong FabellaÎncă nu există evaluări
- HEMATOCHEZIADocument26 paginiHEMATOCHEZIAAlvin HartantoÎncă nu există evaluări
- Abdominal Compartment Syndrome: By: Adel Ghuloom, MD Lubna Kamaldien, MDDocument42 paginiAbdominal Compartment Syndrome: By: Adel Ghuloom, MD Lubna Kamaldien, MDnanang anacardia Subagyo100% (1)
- Abdominal Compartment SyndromeDocument29 paginiAbdominal Compartment Syndromesgod34100% (1)
- GI Bleeding - NursesDocument71 paginiGI Bleeding - Nursesapi-3760283100% (6)
- A Case Study About Upper GastroIntestinal BleedingDocument46 paginiA Case Study About Upper GastroIntestinal BleedingChristal Mae VillaminÎncă nu există evaluări
- Intra Abdominal HypertensionDocument22 paginiIntra Abdominal HypertensionFernando MorenoÎncă nu există evaluări
- PeritonitisDocument42 paginiPeritonitisvriliadiar100% (1)
- Lower GI BleedingDocument3 paginiLower GI BleedingTaleb AliÎncă nu există evaluări
- Prostate CancerDocument6 paginiProstate CancerfheisanzÎncă nu există evaluări
- Presented By: Dr. Siddhant Singh Moderator: Prof. Dr. Sanjay Kala (MS)Document100 paginiPresented By: Dr. Siddhant Singh Moderator: Prof. Dr. Sanjay Kala (MS)Sid Sid100% (3)
- Lower GI Bleeding SlideDocument29 paginiLower GI Bleeding Slideraed faisalÎncă nu există evaluări
- 06prof. Riwanto-Abdominal Compartment SyndromeDocument41 pagini06prof. Riwanto-Abdominal Compartment SyndromeTanujaa Venugopal100% (1)
- Intestinal ObstructionDocument35 paginiIntestinal Obstructionwht89100% (1)
- 2 Acute CholecystitisDocument21 pagini2 Acute CholecystitisEtteh MaryÎncă nu există evaluări
- Topic - Diaphragmatic HerniasDocument13 paginiTopic - Diaphragmatic HerniasOlga CerlatÎncă nu există evaluări
- 21 Obstructive JaundiceDocument12 pagini21 Obstructive JaundicejumaymayaÎncă nu există evaluări
- Cholangitis: Reported By: R. DongaranDocument18 paginiCholangitis: Reported By: R. DongaranVishnu Karunakaran100% (1)
- PEPTIC ULCER DISEASE 2018 EdittedDocument43 paginiPEPTIC ULCER DISEASE 2018 EdittedJumbe MohamedÎncă nu există evaluări
- Sirs & ModsDocument26 paginiSirs & Modsnerlyn silao50% (2)
- Intestinal Obstruction 4Document25 paginiIntestinal Obstruction 4Muvenn KannanÎncă nu există evaluări
- Calculous Biliary DiseaseDocument71 paginiCalculous Biliary DiseaseMinnossÎncă nu există evaluări
- Intestinal Obstruction Due To AdhesionDocument55 paginiIntestinal Obstruction Due To Adhesionadekooluseun100% (6)
- Laparoscopic CholecystectomyDocument100 paginiLaparoscopic CholecystectomyRakshay Kaul100% (1)
- Chest Trauma ManagementDocument78 paginiChest Trauma ManagementHassan Shoukat100% (1)
- Upper GIT BleedingDocument69 paginiUpper GIT BleedingSoleh Ramly100% (1)
- Gastrointestinal EndosDocument28 paginiGastrointestinal EndosAqeel AhmedÎncă nu există evaluări
- Intestinal ObstructionDocument52 paginiIntestinal ObstructionAsfandyar Khan100% (2)
- Urolithiasis Case ReportDocument14 paginiUrolithiasis Case ReportCarl Elexer Cuyugan Ano100% (3)
- Anatomy and Physiology of Biliary TreeDocument48 paginiAnatomy and Physiology of Biliary TreeKamalakanta Das100% (1)
- Cholangitis and Cholecystitis (DR - Dr. Hery Djagat Purnomo, SpPD-KGEH)Document47 paginiCholangitis and Cholecystitis (DR - Dr. Hery Djagat Purnomo, SpPD-KGEH)Aditya SahidÎncă nu există evaluări
- Roru Exoendo - PancreasDocument13 paginiRoru Exoendo - PancreasRitz CelsoÎncă nu există evaluări
- Chole CystDocument12 paginiChole CystMoch NizamÎncă nu există evaluări
- Cholecystitis & Carcinoma of GallbladderDocument37 paginiCholecystitis & Carcinoma of GallbladderSalsabila Al-Basheer100% (1)
- Complete Intestinal ObstructionDocument8 paginiComplete Intestinal ObstructionThuganamix100% (2)
- GI Answer Key Part 1Document5 paginiGI Answer Key Part 1Nom NomÎncă nu există evaluări
- ColostomyDocument60 paginiColostomymathisyncÎncă nu există evaluări
- Acute PancreatitisDocument76 paginiAcute PancreatitisKamran Khan Khalil100% (1)
- Management of Upper Gastrointestinal BleedingDocument62 paginiManagement of Upper Gastrointestinal BleedingAgustinus FatollaÎncă nu există evaluări
- BurnsDocument80 paginiBurnsmarÎncă nu există evaluări
- Chest Tube ThoracostomyDocument43 paginiChest Tube ThoracostomyAhsia LorraineÎncă nu există evaluări
- Achalasia KSDocument40 paginiAchalasia KSPridho GaziansyahÎncă nu există evaluări
- Intestinal ObstructionDocument48 paginiIntestinal ObstructionMahmoud AbuAwadÎncă nu există evaluări
- Upper Gastrointestinal Bleeding (Ugib) : First Shift: August 13, 2018Document10 paginiUpper Gastrointestinal Bleeding (Ugib) : First Shift: August 13, 2018Angelo Dela Cruz VillaromanÎncă nu există evaluări
- Urinary System and Male Genital OrgansDocument28 paginiUrinary System and Male Genital Organsapi-19641337Încă nu există evaluări
- TelencephalonDocument22 paginiTelencephalonapi-19641337Încă nu există evaluări
- Respiratory System5Document24 paginiRespiratory System5api-19641337Încă nu există evaluări
- Spinal Nerves (Lumber Sacral)Document25 paginiSpinal Nerves (Lumber Sacral)api-19641337Încă nu există evaluări
- Spinal Nerves1Document25 paginiSpinal Nerves1api-19641337Încă nu există evaluări
- Urinary System and Male Genital OrgansDocument28 paginiUrinary System and Male Genital Organsapi-19641337Încă nu există evaluări
- Veins: Anatomy Department, School of Medicine, Wuhan UniversityDocument18 paginiVeins: Anatomy Department, School of Medicine, Wuhan Universityapi-19641337Încă nu există evaluări
- Recognization On Section of Spinal CordDocument26 paginiRecognization On Section of Spinal Cordapi-19641337Încă nu există evaluări
- Lower Limb Muscles-20061120Document17 paginiLower Limb Muscles-20061120api-19641337Încă nu există evaluări
- Highlights of The Systemic Anatomy: Important Concepts Important ContentsDocument5 paginiHighlights of The Systemic Anatomy: Important Concepts Important Contentsapi-19641337Încă nu există evaluări
- Three Main Functions:: The Nervous System Is The Master Controlling System of The BodyDocument34 paginiThree Main Functions:: The Nervous System Is The Master Controlling System of The Bodyapi-19641337Încă nu există evaluări
- Introduction and Spinal CordDocument27 paginiIntroduction and Spinal Cordapi-196413370% (1)
- Muscles of Upper Limb: Wang HaoDocument22 paginiMuscles of Upper Limb: Wang Haoapi-19641337100% (2)
- General Discription of MusclesDocument25 paginiGeneral Discription of Musclesapi-19641337Încă nu există evaluări
- Cerebellum & DiencephalonDocument21 paginiCerebellum & Diencephalonapi-19641337Încă nu există evaluări
- Angiology: (Circulatory System)Document40 paginiAngiology: (Circulatory System)api-19641337100% (1)
- EYE&ear 1Document69 paginiEYE&ear 1api-19641337Încă nu există evaluări
- Cranial Nerves (III)Document23 paginiCranial Nerves (III)api-19641337Încă nu există evaluări
- Blood Vessels: Artery Capillary VeinDocument27 paginiBlood Vessels: Artery Capillary Veinapi-19641337Încă nu există evaluări
- Female Genital Organs and PeritoneumDocument16 paginiFemale Genital Organs and Peritoneumapi-19641337Încă nu există evaluări
- Orign and Passage of The Cranial NerveDocument20 paginiOrign and Passage of The Cranial Nerveapi-19641337Încă nu există evaluări
- Bones and Joints of TrunkDocument56 paginiBones and Joints of Trunkapi-196413370% (1)
- Cranial Nerves (I)Document29 paginiCranial Nerves (I)api-19641337Încă nu există evaluări
- Bones and Joints of The Lower Limb.102Document13 paginiBones and Joints of The Lower Limb.102api-19641337Încă nu există evaluări
- 02 SkullDocument19 pagini02 Skullapi-19641337Încă nu există evaluări
- 01introduction SkeletonDocument12 pagini01introduction Skeletonapi-19641337Încă nu există evaluări
- Superior Aspect of Calvaria: Suture Suture SutureDocument11 paginiSuperior Aspect of Calvaria: Suture Suture Sutureapi-19641337Încă nu există evaluări
- 03plactice For SkullDocument2 pagini03plactice For Skullapi-19641337Încă nu există evaluări
- 01skull IndividualBonesDocument10 pagini01skull IndividualBonesapi-19641337Încă nu există evaluări
- Brain Stem 1Document25 paginiBrain Stem 1api-19641337Încă nu există evaluări
- Pod HD500X SMDocument103 paginiPod HD500X SMerendutekÎncă nu există evaluări
- Prepare Active Directory and Domains For Exchange 2013 PDFDocument18 paginiPrepare Active Directory and Domains For Exchange 2013 PDFAdam DanielÎncă nu există evaluări
- Gaffney S Business ContactsDocument6 paginiGaffney S Business ContactsSara Mitchell Mitchell100% (1)
- Introduction To Civics Lesson PlanDocument3 paginiIntroduction To Civics Lesson Planapi-491671554Încă nu există evaluări
- Security Information and Event Management (SIEM) - 2021Document4 paginiSecurity Information and Event Management (SIEM) - 2021HarumÎncă nu există evaluări
- Philsa International Placement and Services Corporation vs. Secretary of Labor and Employment PDFDocument20 paginiPhilsa International Placement and Services Corporation vs. Secretary of Labor and Employment PDFKrissaÎncă nu există evaluări
- Specifications: Back2MaintableofcontentsDocument31 paginiSpecifications: Back2MaintableofcontentsRonal MoraÎncă nu există evaluări
- SSoA Resilience Proceedings 27mbDocument704 paginiSSoA Resilience Proceedings 27mbdon_h_manzano100% (1)
- Ernest Renan What Is Nation PDFDocument2 paginiErnest Renan What Is Nation PDFJohnny0% (1)
- Scott CH 3Document16 paginiScott CH 3RATNIDAÎncă nu există evaluări
- Engg 135 Design of Reinforced Concrete Structures: Bond and Bar Development Reading: Wight and Macgregor Chapter 8Document24 paginiEngg 135 Design of Reinforced Concrete Structures: Bond and Bar Development Reading: Wight and Macgregor Chapter 8Manuel MirandaÎncă nu există evaluări
- The Theory of Paulo FreireDocument8 paginiThe Theory of Paulo FreireLola Amelia100% (3)
- Bennett Et Al 2019 Towards A Sustainable and Equitable Blue EconomyDocument3 paginiBennett Et Al 2019 Towards A Sustainable and Equitable Blue Economynaomi 23Încă nu există evaluări
- First Floor Plan SCALE:1:50: Master BedroomDocument1 paginăFirst Floor Plan SCALE:1:50: Master BedroomRiya MehtaÎncă nu există evaluări
- NLP - Neuro-Linguistic Programming Free Theory Training Guide, NLP Definitions and PrinciplesDocument11 paginiNLP - Neuro-Linguistic Programming Free Theory Training Guide, NLP Definitions and PrinciplesyacapinburgosÎncă nu există evaluări
- Corporation True or FalseDocument2 paginiCorporation True or FalseAllyza Magtibay50% (2)
- Tax Compliance, Moral..Document52 paginiTax Compliance, Moral..PutriÎncă nu există evaluări
- SSD Term 3Document52 paginiSSD Term 3anne_barltropÎncă nu există evaluări
- Los Angeles County Sheriff's Department InvestigationDocument60 paginiLos Angeles County Sheriff's Department InvestigationBen Harper0% (1)
- Measures of Variability For Ungrouped DataDocument16 paginiMeasures of Variability For Ungrouped DataSharonÎncă nu există evaluări
- The Periodontal Ligament: A Unique, Multifunctional Connective TissueDocument21 paginiThe Periodontal Ligament: A Unique, Multifunctional Connective TissueSamuel Flores CalderonÎncă nu există evaluări
- Tieng Anh Thuong Mai 1Document18 paginiTieng Anh Thuong Mai 1nminhvan072Încă nu există evaluări
- Lesson On Inferring Tone and MoodDocument32 paginiLesson On Inferring Tone and MoodAngel PabilloÎncă nu există evaluări
- Composition Notes Essay C1 and C2Document7 paginiComposition Notes Essay C1 and C2Γιάννης ΜατσαμάκηςÎncă nu există evaluări
- I. Lesson Plan Overview and DescriptionDocument5 paginiI. Lesson Plan Overview and Descriptionapi-283247632Încă nu există evaluări
- Week 5 Class 2Document33 paginiWeek 5 Class 2ppÎncă nu există evaluări
- Alliance Manchester Business SchoolDocument14 paginiAlliance Manchester Business SchoolMunkbileg MunkhtsengelÎncă nu există evaluări
- Study of Indian Wrist Watch Industry and Repositioning Strategy of Titan WatchesDocument60 paginiStudy of Indian Wrist Watch Industry and Repositioning Strategy of Titan WatchesVinay SurendraÎncă nu există evaluări
- Angels We Have Heard On High PDFDocument2 paginiAngels We Have Heard On High PDFEmerson Joseph BautistaÎncă nu există evaluări
- Research Papers Harvard Business SchoolDocument8 paginiResearch Papers Harvard Business Schoolyquyxsund100% (1)